Downloaded 77 times








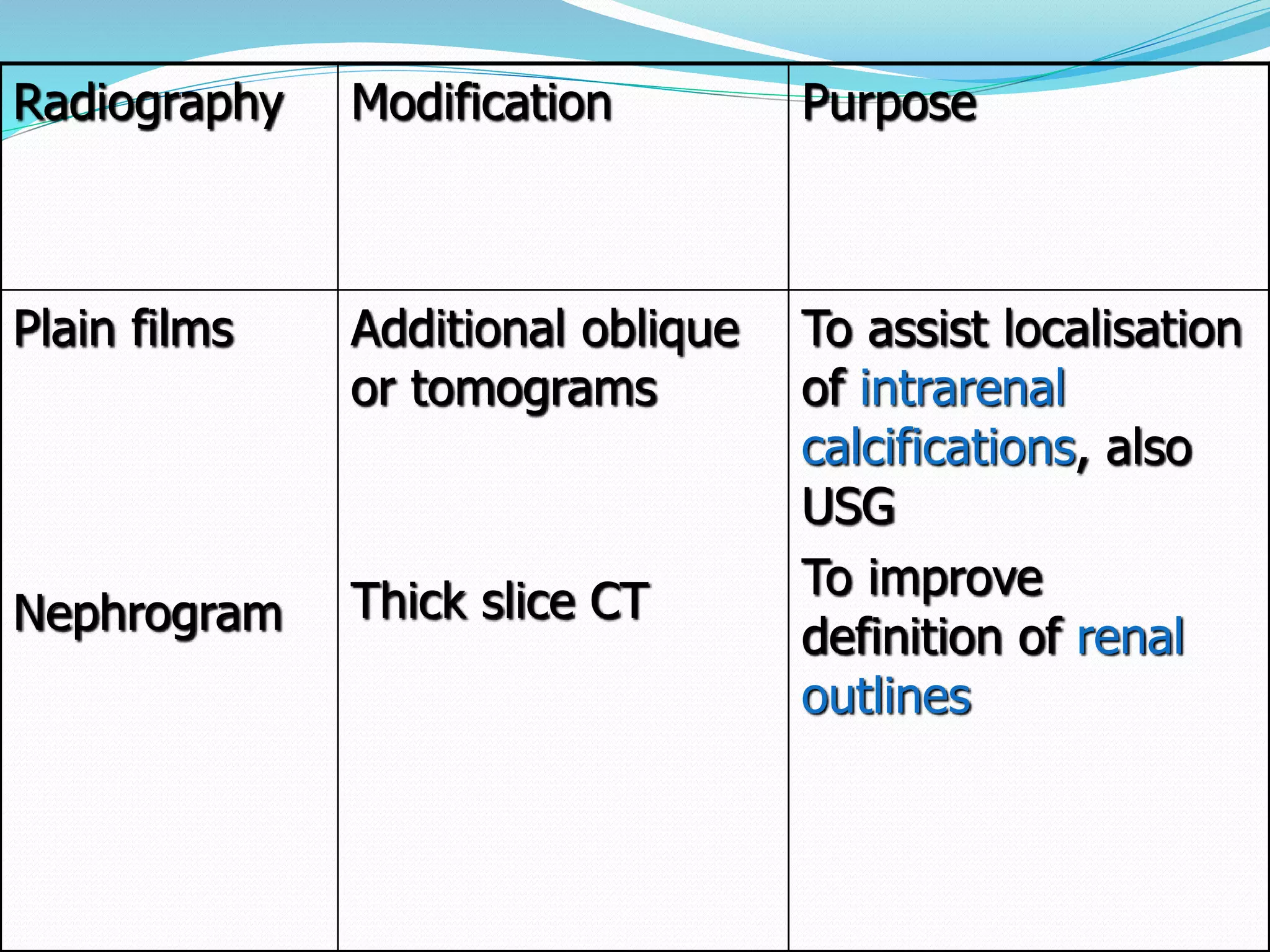
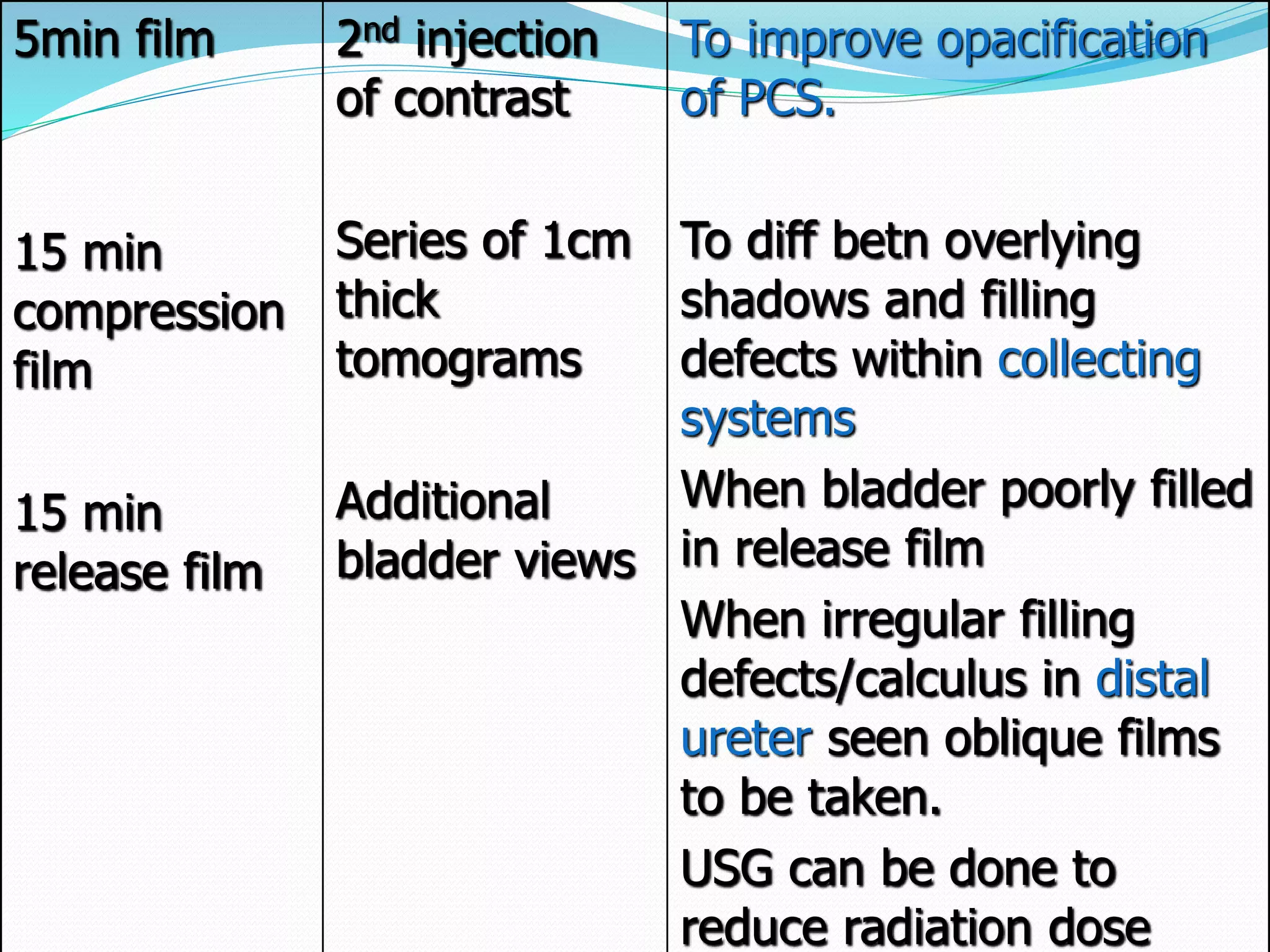
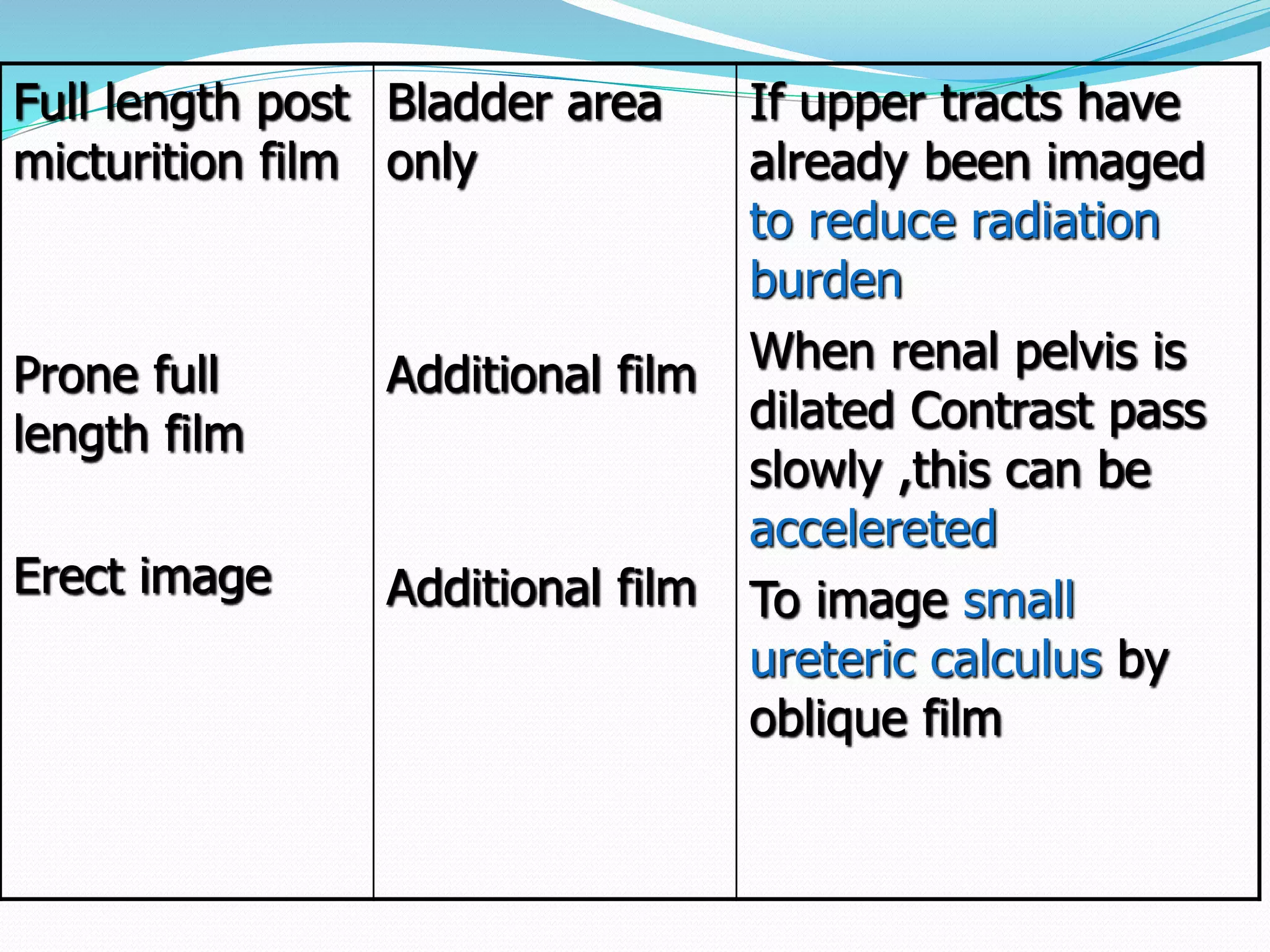
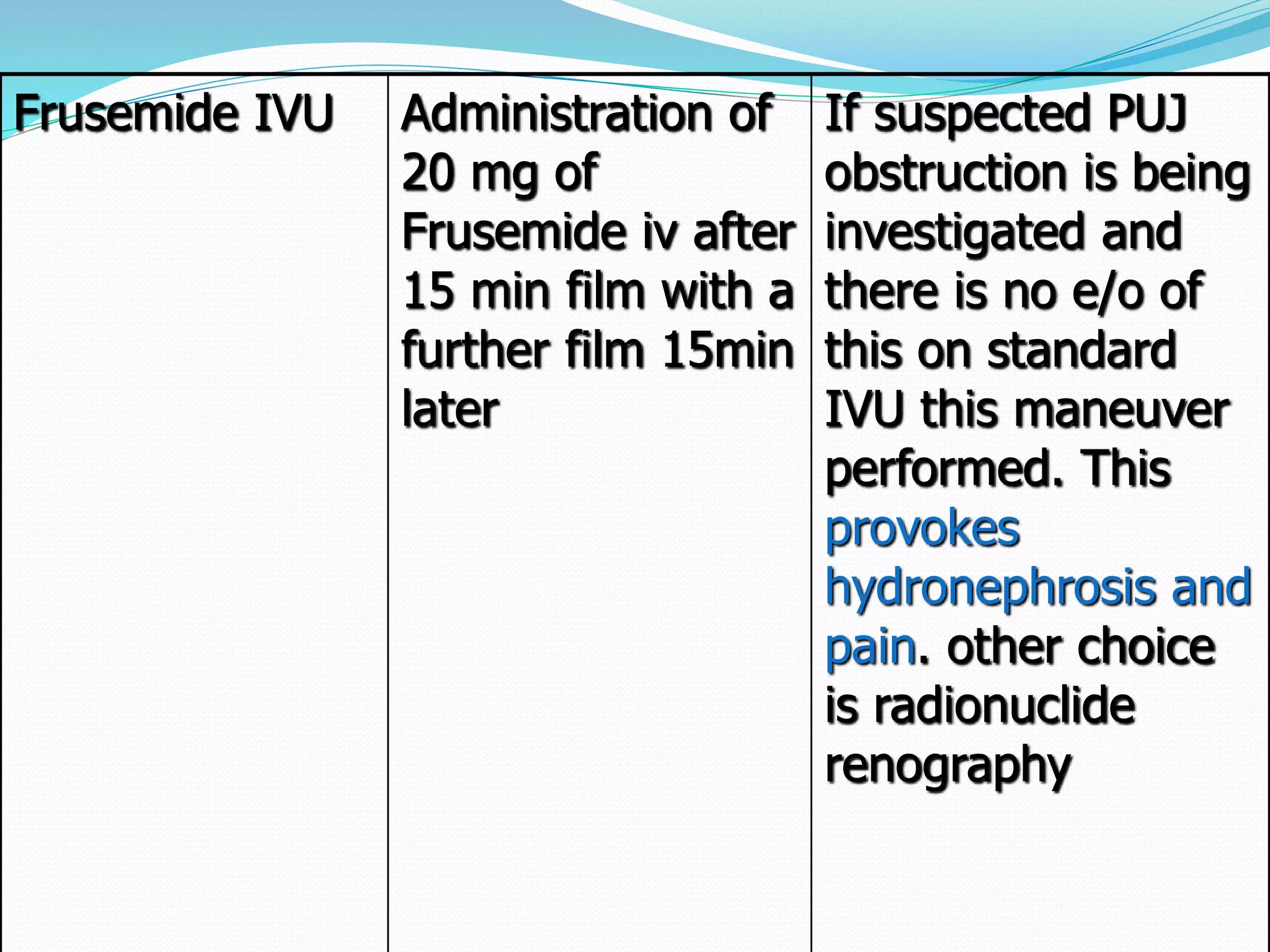







This document provides an overview of intravenous urography (IVU), including indications, contraindications, technique, projections, and modifications. IVU involves intravenous injection of contrast medium to visualize the urinary tract. It is declining in use due to newer modalities like CT and MRI, adverse effects of contrast, and cost. The document outlines patient preparation, standard projections including nephrogram, 5-minute, compression, and post-void films. It also discusses non-routine projections, contrast agents, and radiation protection. Complications and aftercare are briefly mentioned.