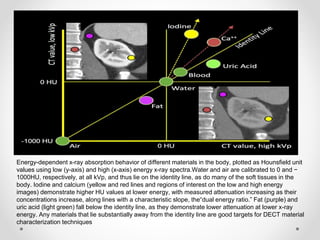
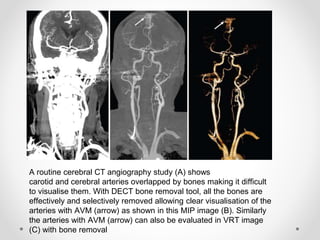
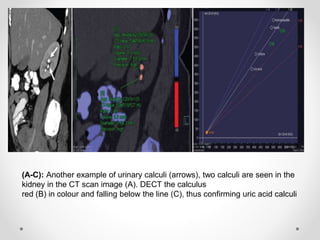
Dual energy CT uses two x-ray spectra to distinguish materials based on their differential attenuation properties. This allows reconstruction of various image sets and material-specific images without contrast. Key applications include bone removal, virtual non-calcium imaging, uric acid stone differentiation, gout detection, perfusion imaging, and differentiating enhancing lesions from calcification. Dual energy CT provides material-specific information useful for diagnosis and treatment planning in various clinical contexts.





































![[5]Isotope_Scan_Surgical_Diseases](https://cdn.slidesharecdn.com/ss_thumbnails/1664464-thumbnail.jpg?width=640&height=640&fit=bounds)































