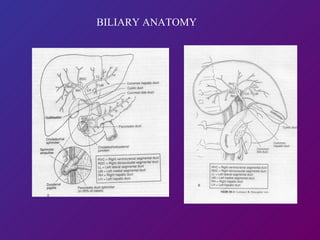
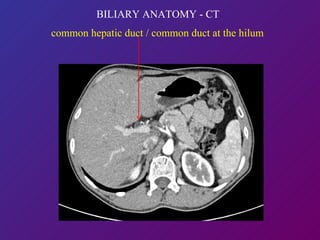
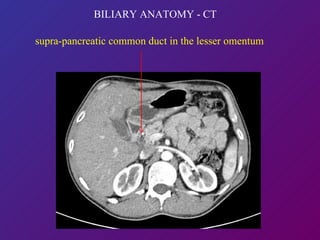
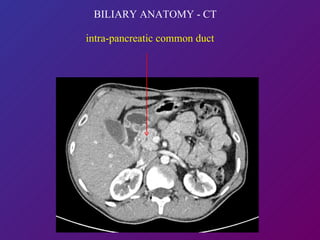
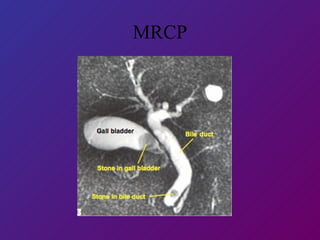
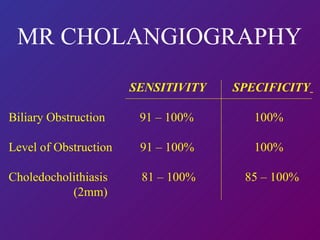
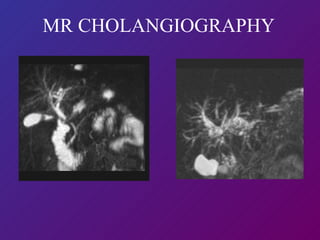
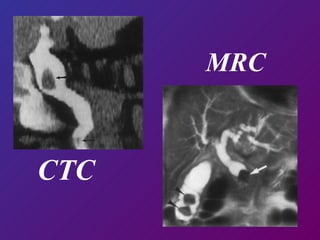
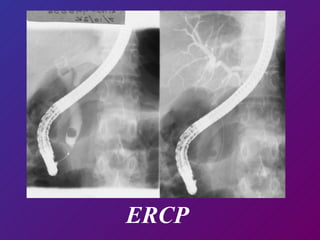
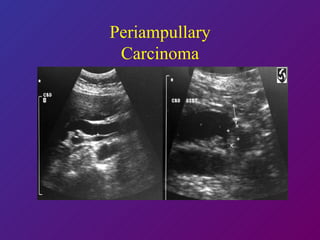
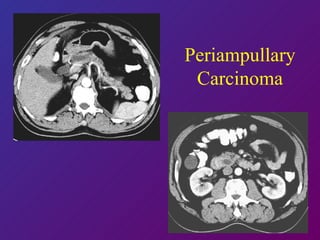
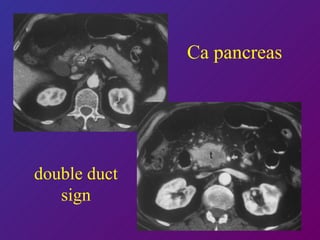
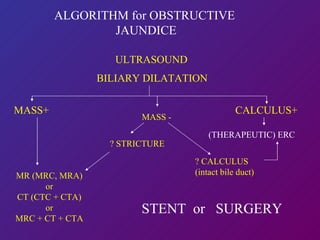
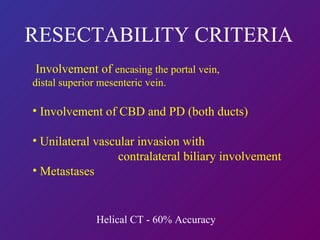
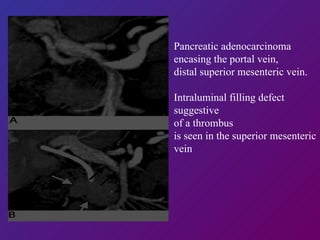
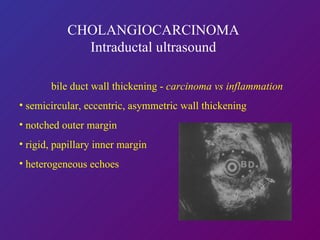
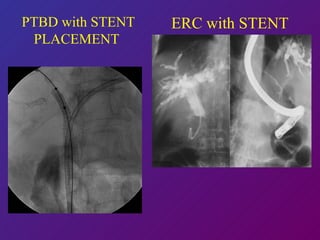
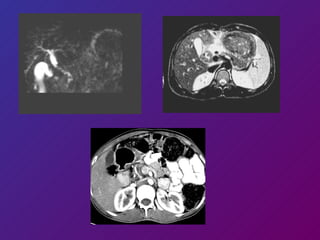
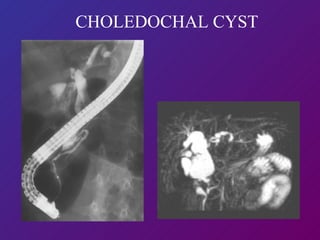
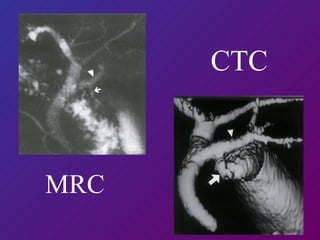
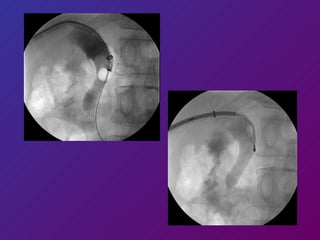
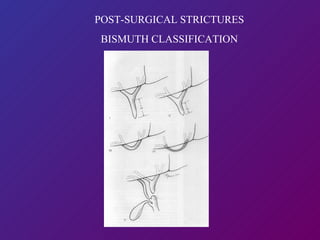
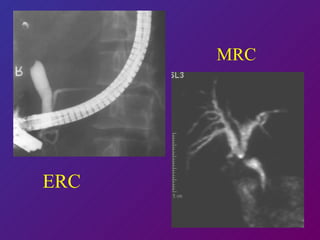
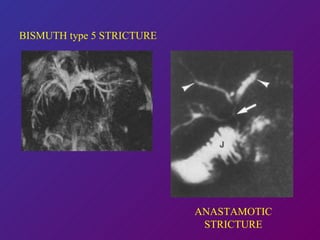
This document discusses the imaging of bile ducts and causes of lower biliary obstruction. It covers the normal biliary anatomy, various imaging modalities used including ultrasound, CT, MRI, ERCP and their appearances. It describes the classification, appearances and algorithms for evaluating obstructive jaundice and discusses specific conditions like choledocholithiasis, cholangiocarcinoma, pancreatic carcinoma and post-surgical complications.