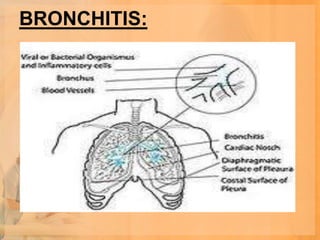
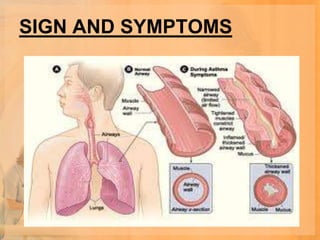
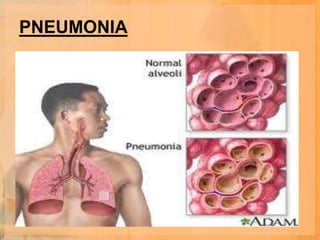
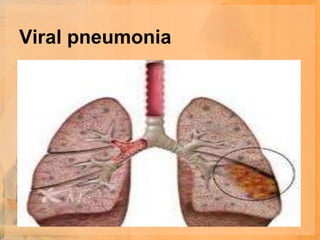
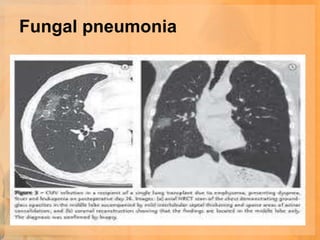
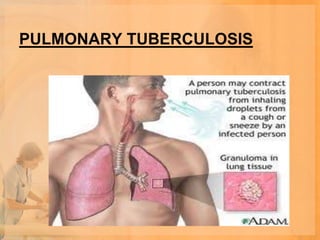
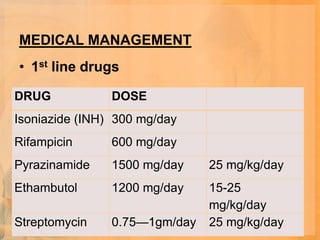
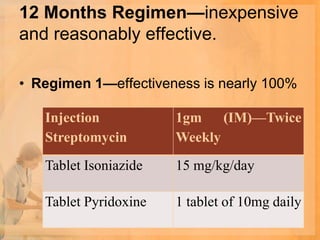
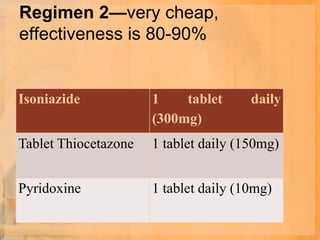
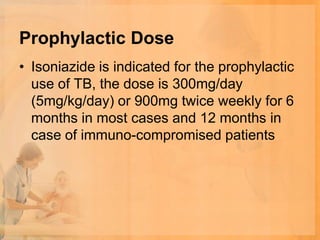
This document provides information on lower respiratory tract infections including bronchitis, pneumonia, and pulmonary tuberculosis. It defines each condition and discusses causes, risk factors, signs and symptoms, diagnostic testing, medical management, nursing management, and prevention. Bronchitis is inflammation of the bronchial tubes caused by viruses or bacteria. Pneumonia is inflammation of the lungs that can be bacterial, viral, or fungal in origin. Pulmonary tuberculosis is a chronic lung infection caused by the bacterium Mycobacterium tuberculosis. Standard treatments and preventative measures are outlined for each condition.