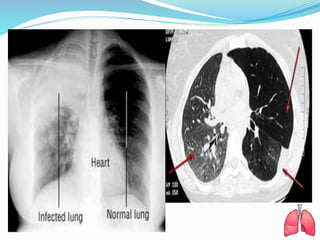
Pneumonia is an inflammatory condition of the lungs caused by microbial agents like bacteria, viruses, and fungi. It affects millions of people worldwide annually and is a common cause of death, especially in young children and older adults. Symptoms include cough, fever, shortness of breath, and chest pain. Diagnosis involves physical exam, chest x-ray, and tests of respiratory samples. Treatment focuses on antibiotics targeting the causative organism as well as oxygen therapy, breathing exercises, and ensuring adequate nutrition and hydration. Complications can include lung abscesses, empyema, and respiratory failure. With treatment, most cases stabilize within a week but full recovery may take several weeks.

![3. Risk for Infection related to inadequate primary defenses due to
decreased ciliary action, stasis of body fluids [respiratory
secretions]; Inadequate secondary defenses due to [presence of
existing infection], immunosuppression; chronic disease,
malnutrition, possibly evidenced By presence of signs and
symptoms establishes an actual diagnosis.
INTERVENTION
Monitor vital signs closely, especially during initiation of
therapy.
Instruct client concerning the disposition of secretions
reporting changes in color, amount, and odor of secretions.
Change position frequently and provide good pulmonary toilet,.
perform proper suctioning technique for ventilated clients as
appropriate.
Limit visitors, and institute isolation precautions as
individually appropriate.](https://image.slidesharecdn.com/pneumoniaseminarpresentaation-181023060755/85/Pneumonia-seminar-presentaation-32-320.jpg)
![5. Acute Pain related to Injuring agents (e.g., biological—
inflammation of lung parenchyma, cellular reactions to
circulating toxins; physical—persistent coughing) possibly
evidenced by Verbal/coded report [pleuritic chest pain,
headache, muscle or joint pain] and guarded behavior,
expressive behavior—restlessness.
INTERVENTION
Determine pain characteristics, Investigate changes in
character, location, and intensity of pain.
Monitor vital signs.
Provide comfort measures, such as back rubs, change of
position, and quiet music or conversation. Encourage use of
relaxation and breathing exercises.
Instruct and assist client in chest-splinting techniques
during coughing episodes.
Administer analgesics and antitussives, as indicated.](https://image.slidesharecdn.com/pneumoniaseminarpresentaation-181023060755/85/Pneumonia-seminar-presentaation-35-320.jpg)