Management of PatientsWith Chest
and Lower Respiratory Tract
Disorders
UNIVERSITY OF DETROIT MERCY
McAuley School of Nursing
NUR 3200
MedSurg I
Chapter 19
Course Faculty: Dr. Wilfred M. Allen
2.
Atelectasis
Closure orcollapse of alveoli
Acute or chronic
Most common is acute atelectasis, which occurs in
the postoperative setting
Symptoms: insidious, increasing dyspnea, cough, and
sputum production
Acute: tachycardia, tachypnea, pleural pain, and
central cyanosis if large areas of the lung are affected
Chronic: similar to acute, pulmonary infection may
be present
3.
Assessment and Diagnosisfor
Atelectasis
Characterized by increased work of breathing and
hypoxemia
Decreased breath sounds and crackles over the
affected area
Chest x-ray may suggest a diagnosis of atelectasis
before clinical symptoms appear
Pulse oximetry (SpO2) may demonstrate a low
saturation of hemoglobin with oxygen (less than
90%)
4.
Nursing Interventions for
Atelectasis
Prevention
Frequent turning
Early mobilization
Strategies to expand lungs and manage secretions
Incentive spirometer
Voluntary deep breathing
Secretion management
Pressurized metered-dose inhaler
5.
Management of Atelectasis
Improve ventilation and remove secretions
First line measures:
‐
Frequent turning, early ambulation, lung volume
expansion maneuvers and coughing
Multidisciplinary: ICOUGH (see Chart 19 3)
‐
PEEP, CPAB, bronchoscopy
CPT
Endotracheal intubation and mechanical ventilation
Thoracentesis to relieve compression
Acute Tracheobronchitis
Inflammationof the mucous membranes of the
trachea usually after a viral infection
Pathophysiology
Mucopurulent sputum
Clinical manifestations
Initially dry cough with mucoid sputum
As progresses, dyspnea, stridor, wheezes, purulent
sputum
8.
Management of Acute
Tracheobronchitis
Medical management
Antibiotics
Analgesics
Increased fluid intake
Cool vapor therapy or steam inhalations
Suctioning
Nursing Management
Bronchial hygiene
Rest
Complete full course of medications
9.
Pneumonia
Inflammation ofthe lung parenchyma caused by
various microorganisms, including bacteria,
mycobacteria, fungi, and viruses
Classification
Community-acquired (CAP)
Health care–associated (HCAP)
Hospital-acquired (HAP)
Ventilator-associated (VAP)
Refer to Chart 19-4
10.
Types of Pneumonia
Community-acquired
Community setting or within first 48 hours post
hospitalization
Rate of infection increases with age
S. Pneumoniae is the most common cause among adults
Viral origin in infants and children
Health care–associated
Often caused by multidrug resistant organisms
‐
Early diagnosis and treatment are critical
11.
Types of Pneumonia
Hospital-acquired
Develops 48 hours or more after hospitalization
Subtype of health care–associated pneumonia
Potential for infection from many sources
High mortality rate
Colonization by multiple organisms due to overuse of
antimicrobial agents
Pleural effusion, high fever, and tachycardia
Common with debilitated, dehydrated patients with
minimal sputum production
12.
Types of Pneumonia
Ventilator-associated
Received mechanical ventilation for at least 48 hours
Prevention is key
VAP bundles (Chart 19-6)
Pneumonia in the immunocompromised host
Common agents include pneumocystis, fungi, and
tuberculosis
Receiving immunosuppressive agents, history of
immunosuppressive condition
Subtle onset with progressive dyspnea, fever, and
nonproductive cough
13.
Pneumonia Risk Factors
Refer to Table 19-2
Occurs in patients with certain underlying disorders
and diseases
Heart failure, diabetes, alcoholism, COPD, and
AIDS
Influenza
Cystic fibrosis
14.
Clinical Manifestations of
Pneumonia
Varies depending on type, causal organism, and
presence of underlying disease
Streptococcal: Sudden onset of chills, fever, pleuritic
chest pain, tachypnea, and respiratory distress
Viral, mycoplasma, or Legionella: relative bradycardia
Other: Respiratory tract infection, headache, low-grade
fever, pleuritic pain, myalgia, rash, and pharyngitis
Orthopnea, crackles, increased tactile fremitus, purulent
sputum
15.
Assessment and Diagnosisof
Pneumonia
History
Physical exam
Chest x-ray
Blood culture
Sputum examination
Bronchoscopy may be used for acute severe infection
16.
Pneumonia Prevention
Pneumococcalvaccination
Reduces the incidence of pneumonia,
hospitalizations for cardiac conditions, and deaths
in the older adult population
Two types of pneumococcal vaccine
Recommended for all adults 65 years of age or
older and 19 years or older with conditions that
weaken the immune system
Other preventive measures, see Table 19-2
17.
Medical Management of
Pneumonia
Administration of the appropriate antibiotic as
determined by the results of a culture and sensitivity
Supportive treatment includes fluids, oxygen for
hypoxia, antipyretics, antitussives, decongestants,
and antihistamines
Antibiotics not indicated for viral infections but are
used for secondary bacterial infection
Refer to Table 19-3
Gerontologic considerations
18.
COVID-19 Considerations
SARS-CoV-2
Asymptomatic to severe viral pneumonia
Fatigue, myalgia, congestion, sore throat, diarrhea,
anosmia, and ageusia
Mostly conservative outpatient management (rest,
hydrate, antipyretic agents)
Hospitalization for severe illness with pneumonia,
increased risk of venous thromboembolism
Can lead to shock and respiratory failure
19.
Assessment of thePatient with
Bacterial Pneumonia
Vital signs
Secretions: amount, odor, color
Cough: frequency and severity
Tachypnea, shortness of breath
Inspect and auscultate chest
Changes in mental status, fatigue, edema,
dehydration, concomitant heart failure, especially in
older adult patients
20.
Problems/Complications of thePatient
with Bacterial Pneumonia
Continuing symptoms after initiation of
therapy
Sepsis and septic shock
Respiratory failure
Atelectasis
Pleural effusion
Delirium
21.
Planning and Goalsfor the Patient with
Bacterial Pneumonia
Improved airway patency
Increased activity
Maintenance of proper fluid volume
Maintenance of adequate nutrition
Understanding of the treatment protocol and
preventive measures
Absence of complications
Based on patient outcomes plan for home,
community, and transitional care
22.
Nursing Interventions forthe Patient with
Bacterial Pneumonia
Oxygen with
humidification to
loosen secretions
Face mask or nasal
cannula
Coughing techniques
Chest physiotherapy
Position changes
Incentive spirometry
Nutrition
Hydration
Rest
Activity as tolerated
Patient education
Self-care
23.
Expected Outcomes forthe Patient with
Bacterial Pneumonia
Demonstrates improved airway patency
Rests and conserves energy and then slowly
increasing activities
Maintains adequate hydration; adequate dietary
intake
Verbalizes increased knowledge about management
strategies
Complies with management strategies
Exhibits no complications
24.
Aspiration
Inhalation offoreign material into the lungs leads to
inflammatory reaction, hypoventilation, and
ventilation–perfusion mismatch
Serious complication is broncho or lobar pneumonia
Risk factor is LOC; refer to Chart 19-8
Key pathophysiology is the volume and character of
aspirated contents (most often GI contents)
25.
Aspiration Prevention
Swallowingscreening
Nursing interventions
Keep HOB elevated and endotracheal cuff elevated
(if intubated)
Avoid stimulation of gag reflex with suctioning or
other procedures
Check for placement before tube feedings
Soft diet, small bites, no straws
Refer to Chart 19-9
26.
Pulmonary Tuberculosis
Mycobacteriumtuberculosis bacillus (TB)
10 million people with TB worldwide and 9,105 cases in the
United States (2017)
Spreads by airborne transmission through droplets then moves
to other parts of the body such as the kidneys, bones, and
cerebral cortex.
Granulomas and Ghon tubercule
Risk factors for TB, refer to Chart 19-10
Low grade fever
‐
Cough; nonproductive or mucopurulent; hemoptysis
Night sweats, fatigue, weight loss
27.
Assessment and Diagnostic
Findingsfor TB
History and physical
TB skin test; Mantoux method: See Figure 19-3
Significant versus nonsignificant reactions
TB blood tests
Sputum culture
Sputum testing
28.
Medical Management ofTB
Treated for 6 to 12 months
Drug resistance is primary concern
Initiate treatment with four or more medications
Complete all therapy
Initial treatment phase (8 weeks)
Continuation phase (4 to 7 months)
Table 19-4
29.
Nursing Management ofTB
Promoting airway clearance
Advocating adherence to the treatment
regimen
Promoting activity and nutrition
Preventing transmission
30.
Lung Abscess
Mostare a complication of bacterial pneumonia
Symptoms vary from a mild productive cough to acute
illness; plueral friction rub
Site of lung abscess related to gravity and determined by
position
Can lead to empyema, bronchopleural fistula
Symptoms vary from a mild productive cough to acute
illness, productive cough with foul sputum, leukocytosis,
pleurisy, dyspnea, weakness, anorexia, and weight loss
31.
Assessment and Diagnostic
Findingsfor Lung Abscess
Pleural friction rub
Crackles
Chest x-ray
Sputum culture
Bronchoscopy
CT of the chest
32.
Medical Management ofLung
Abscess
Prevention
Adequate drainage of the lung
Chest physiotherapy
Diet high in protein and calories
Antimicrobial therapy
Pulmonary resection (rare)
33.
Nursing Management ofLung
Abscess
Administer IV antibiotics for 3 to 5 days, followed
by oral antibiotics for 4 to 12 weeks
CPT
Educate patient to perform deep breathing and
coughing exercises
Encourage diet high in protein and calories
Emotional support
Promote home, community-based, and transitional
care
34.
Sarcoidosis
Occurs between20 and 40 years of age
More common in African American women
Interstitial lung disease that is inflammatory,
multisystem, granulomatous with unknown origin
(any organ may be affected)
Clinical picture depends on systems affected
including dyspnea, cough, hemoptysis, congestion,
anorexia, fatigue, and weight loss
35.
Assessment and Diagnostic
Findingsfor Sarcoidosis
Chest x-ray and CT scans
Mediastinoscopy or transbronchial biopsy
Pulmonary function test
Arterial blood gases
Need biopsy for definitive diagnosis
36.
Management of Sarcoidosis
Medical management
Corticosteroids
May have spontaneous remission without treatment
Immune modulator
Nursing management
Support all medical treatments
Patient education for medication and when to notify the primary
provider
Chronic illness management
Contact Foundation for Sarcoidosis Research for community
resources
37.
Pleural Conditions
Disordersthat involve
The membranes covering the lungs (visceral
pleura) and the surface of the chest wall (parietal
pleura)
Disorders affecting the pleural space
Pleurisy
Pleural effusion
Empyema
Pulmonary edema
38.
Pleurisy
Inflammation ofboth layers of pleurae
Key characteristic of pleuritic pain is its relationship to
respiratory movement
Pleural friction rub can be heard with the stethoscope
Diagnostic tests may include chest x-rays, sputum
analysis, thoracentesis
Treat underlying cause, provide analgesia, teaching to
splint the rib cage when coughing
39.
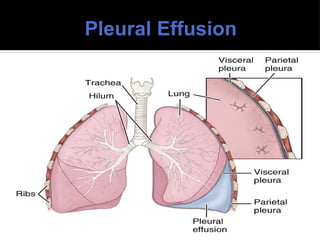
Pleural Effusion
Fluidcollection in pleural space usually secondary to heart failure, TB,
pneumonia, pulmonary infections
Fever, chills, pleuritic pain, dyspnea (large effusion)
Decreased or absent breath sounds; decreased fremitus; and a dull, flat
sound on percussion
May have tracheal deviation away from affected side
Chest x-ray, chest CT, and thoracentesis (fluid analysis)
Treat underlying cause
Pleurodesis
Nurse must support the medial regimen and provide patient and family
education
Empyema
Accumulation ofthick, purulent fluid in pleural space
Complication of bacterial pneumonia or lung abscess
Acutely ill and has signs and symptoms similar to those of an
acute respiratory infection or pneumonia
Chest auscultation demonstrates decreased or absent breath
sounds over the affected area
Chest CT and a diagnostic thoracentesis
Drain fluid and administer antibiotics for 4 to 6 weeks
Nursing management focused on psychosocial support and
lung-expanding breathing exercises
42.
Acute Respiratory Failure
Rapid deterioration to hypoxemia, hypercapnia, and
respiratory acidosis
Impaired ventilation of perfusion mechanisms
Early signs: restlessness, tachycardia, hypertension,
fatigue, headache
Later signs: confusion, lethargy, central cyanosis,
diaphoresis, respiratory arrest
Clinical manifestations: use of accessory muscles,
decreased breath sounds
43.
Medical and NursingManagement
of ARF
Identification and treatment of underlying cause
Intubation, mechanical ventilation
Nutritional support, enteral feedings preferred
Reduce anxiety
Provide patient a form of communication
Prevent complications (turning, ROM, mouth care,
skin care)
44.
Endotracheal Intubation
Passingan endotracheal tube through the nose or mouth
into the trachea (Figure 19-5)
Provides patent airway, access for mechanical
ventilation, facilitates removal of secretions
Nursing care, refer to Chart 19-12
Maintain cuff pressure between 20 and 25 mm Hg
Intubation for no longer than 14 to 21 days (after will
require a tracheostomy)
45.
Tracheotomy
Surgical procedurein which an opening is made into
the trachea
The indwelling tube inserted into the trachea is called
a tracheostomy tube (stoma may be temporary or
permanent) (Fig. 19-6)
Preventing complications associated with
endotracheal and tracheostomy tubes, refer to Chart
19-13
46.
Nursing Management of
Tracheostomy
Continuous monitoring and assessment
Maintain patency by proper suctioning
Semi-Fowler
Administer analgesia and sedatives
Provide an effective means of communication
Suctioning guidelines
Educate patient and family about daily care and how
to prevent an emergency
47.
Mechanical Ventilation
Positiveor negative pressure device to maintain
ventilation and oxygenation for a prolonged period
General indications, refer to Chart 19-14
Classification of ventilators
Ventilator modes, see Figure 19-8
Ventilator settings, refer to Chart 19-15
Weaning the patient from the ventilator, refer to
Chart 19-19
48.
Noninvasive Positive-Pressure
Ventilation
Methodof positive-pressure ventilation that can be
given via facemasks that cover the nose and mouth,
nasal masks, or other oral or nasal devices such as the
nasal pillow
Eliminates need for endotracheal intubation or
tracheostomy
Continuous positive airway pressure (CPAP)
Bilevel positive airway pressure (BiPAP)
Indications: respiratory arrest, serious dysrhythmias,
cognitive impairment, head/facial trauma
49.
Assessment of thePatient Receiving
Mechanical Ventilation
Systematic assessment of all body systems:
In-depth respiratory assessment including all
indicators of oxygenation status
Neurologic status
Effective coping and emotional needs
Comfort level and ability to communicate needs
Assessment of the equipment and settings
Alarm fatigue
50.
Problems/Complications of thePatient
Receiving Mechanical Ventilation
Ventilator problems
Alterations in cardiac function
Barotrauma and pneumothorax
Pulmonary infection and sepsis
Delirium and post-intensive care syndrome
51.
Planning and Goalsfor the Patient
Receiving Mechanical Ventilation
Goals include:
Maintenance of patent airway
Optimal gas exchange
Absence of trauma or infection
Attainment of optimal mobility
Adjustment to nonverbal methods of
communication
Successful coping measures
52.
Nursing Interventions forthe Patient
Receiving Mechanical Ventilation
Enhancing gas exchange
Promoting effective airway clearance
Preventing injury and infection
Promoting optimal level of mobility
Promoting optimal communication
Promoting coping ability
53.
Nursing Intervention: Enhancing
GasExchange
Judicious use of analgesics to relieve pain without
suppressing respiratory drive
Frequent repositioning to diminish the pulmonary
effects of immobility
Monitor for adequate fluid balance:
Assess peripheral edema
I&O and daily weights
Administer medications to control primary disease
54.
Nursing Intervention: Promoting
EffectiveAirway Clearance
Assess lung sounds at least every 2 to 4 hours
Measures to clear airway: suctioning, CPT, position
changes, promote increased mobility
Humidification of airway
Administer medications
Bronchodilators
Mucolytics
Suctioning only if excessive secretions
Other Interventions forthe Patient
Receiving Mechanical Ventilation
ROM and immobility
Communication methods
Stress reduction techniques
Interventions to promote coping
Include in care: family teaching, and the emotional
and coping support of the family
Nutrition
Home and transitional care, refer to Charts 19-17 and
19-18
57.
Acute Respiratory Distress
Syndrome(ARDS)
Mortality rate of 27% to 50%
Characterized by sudden, progressive pulmonary edema,
increasing bilateral lung infiltrates visible on chest x-ray,
and absence of an elevated left atrial pressure
Refer to Figure 19-9
Rapid onset of severe dyspnea and V/Q mismatch <72
hours after precipitating event
Classified by severity of hypoxemia that does not respond
to supplemental oxygen therapy
Crackles, intercostal retractions and BNP levels
58.
Medical Management ofARDS
Identification and treatment of underlying cause
Intubation, mechanical ventilation with PEEP to
keep alveoli open
Treat hypovolemia to keep hemodynamically stable
Prone positioning is best for oxygenation, frequent
repositioning to safeguard integumentary system
Nutritional support, enteral feedings preferred
Reduce anxiety, sedation, paralysis
Supportive care
Occupational Lung Disease:
Pneumoconioses
Includes asbestosis, silicosis, and coal workers’ pneumoconiosis
Refers to a nonneoplastic alteration of the lung resulting from
inhalation of mineral or inorganic dust
Preventable, not treatable
Reduce exposure, protective gear/devices
Role of nurse is to be the employee advocate and provide health
education on preventive measures to reduce lung injury
Assessment: exposure to agent, length of time exposed to onset
of symptoms, congruence of symptoms
Refer to Table 19-6
65.
Lung Cancer
Leadingcause of cancer death in the United States
>85% caused by cigarette smoke
Classification (cell type): 13% SCLC and 84% NSCLC
tumors
Staging: size, location, lymph node involvement,
metastasis (refer to Table 19-7)
Often asymptomatic until late stage
Treatment:
Surgery, radiation, chemotherapy, immunotherapy
Nurse navigators (palliative care)
66.
Nursing Care ofthe Patient with
Lung Cancer
Strategies to ensure relief of pain and discomfort and
prevent complications
Managing symptoms
Dyspnea, fatigue, nausea and vomiting, anorexia
Relieving breathing problems
Airway clearance techniques
Reducing fatigue
Psychological support
67.
Preoperative Management ofthe
Patient Having a Thoracotomy
Assessment and diagnosis
Improving airway clearance
Educating the patient
Forced expiratory technique, diaphragmatic and
pursed-lip breathing
Relieving anxiety
68.
Postoperative Management ofthe Patient
Having a Thoracotomy
Vital signs checked frequently, monitor for
complications
Oxygen
Elevate HOB 30 to 45 degrees
Careful positioning
Medication for pain
Mechanical ventilation
Chest drainage
Refer to Charts 19-23 and 19-25
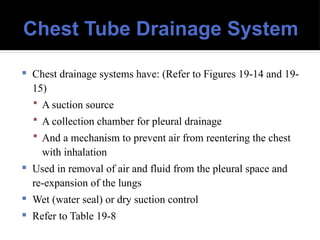
Chest Tube DrainageSystem
Chest drainage systems have: (Refer to Figures 19-14 and 19-
15)
A suction source
A collection chamber for pleural drainage
And a mechanism to prevent air from reentering the chest
with inhalation
Used in removal of air and fluid from the pleural space and
re-expansion of the lungs
Wet (water seal) or dry suction control
Refer to Table 19-8













































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



