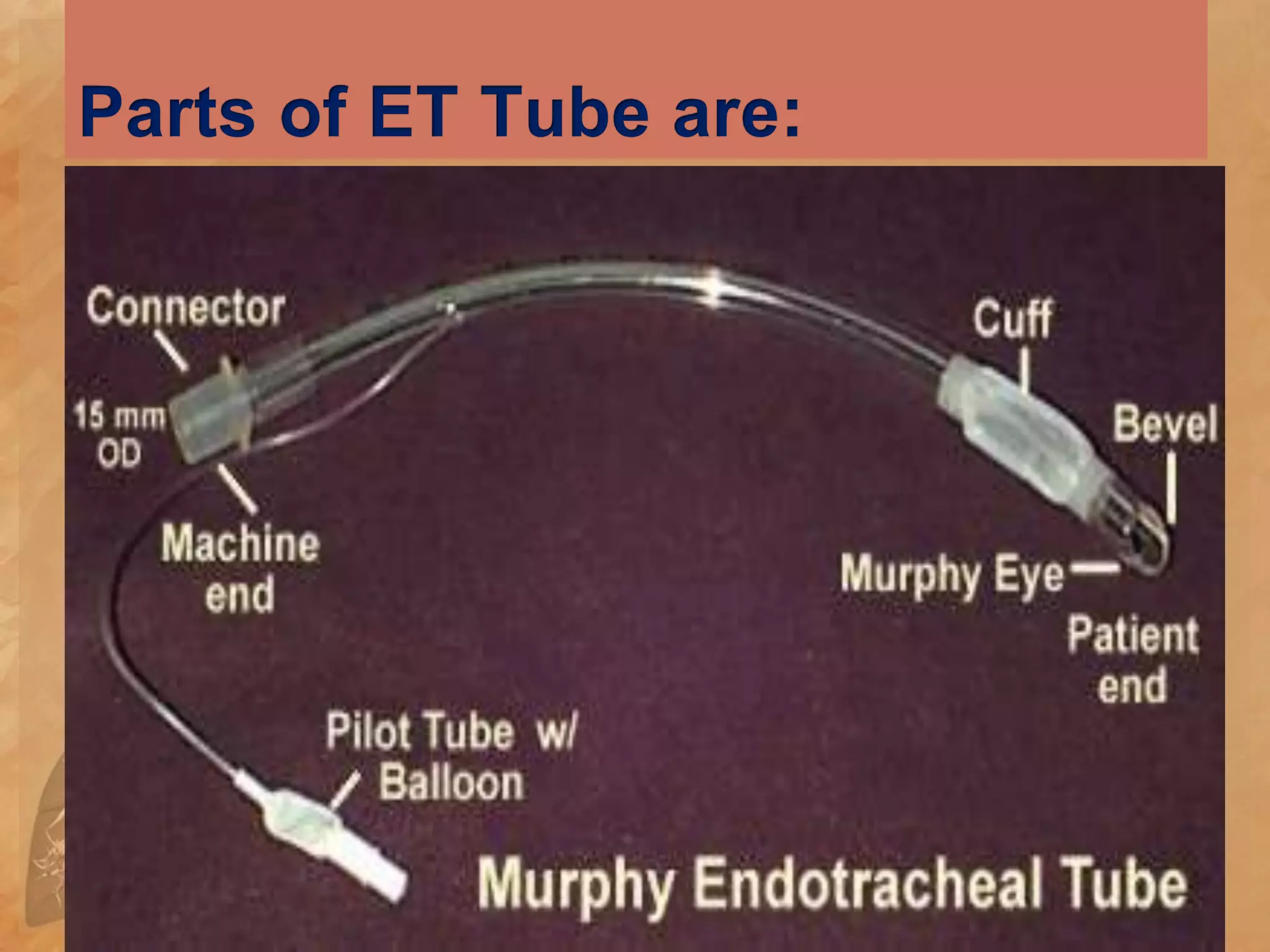
Endotracheal suctioning involves mechanically aspirating pulmonary secretions from patients with an artificial airway. It is done to maintain a clear airway, improve oxygenation, stimulate coughing, and prevent infections. Signs that suctioning is needed include abnormal breath sounds, increased pressures during ventilation, inability to cough effectively, or deteriorating blood gases. Risks include hypoxemia, infection, and trauma, so nurses assess patients' tolerance of the procedure and position them comfortably before carefully performing suctioning with sterile technique.