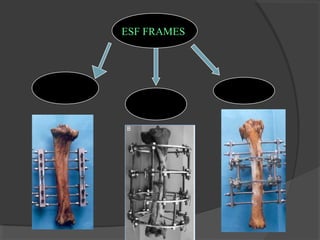
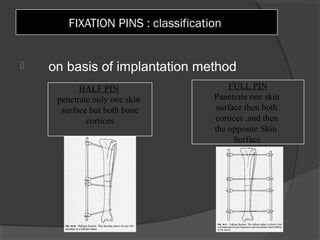
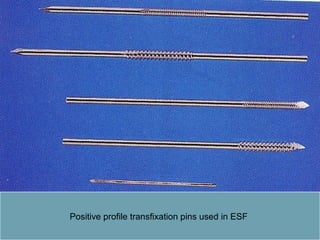
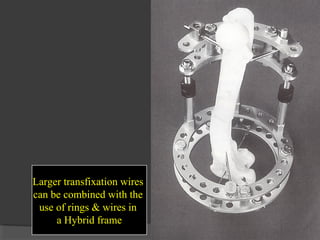
External skeletal fixation techniques involve the percutaneous placement of transcortical pins or wires externally connected to a rigid frame to stabilize fractures. It provides minimally invasive stabilization while preserving blood supply, with advantages of immediate weight bearing and joint mobility. Disadvantages include the need for regular cleaning and monitoring to prevent infection, and higher costs compared to internal fixation. Various configurations and equipment like pins, rings, connectors are used for different applications like fracture fixation, limb lengthening, and deformity corrections.