Downloaded 49 times
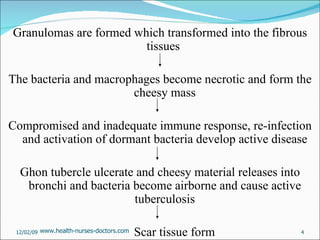
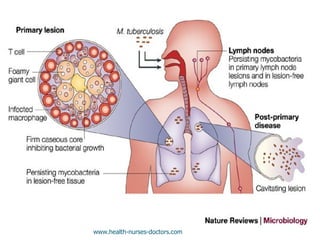
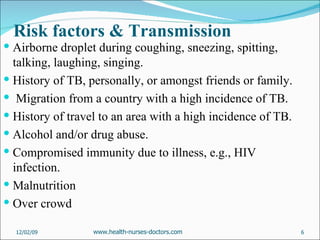
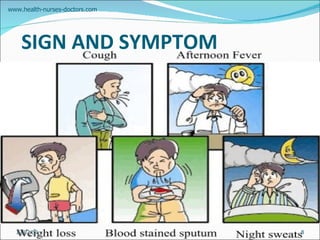
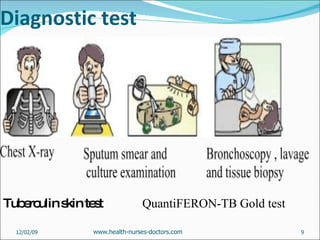
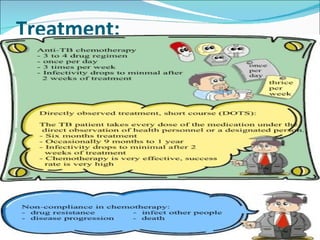
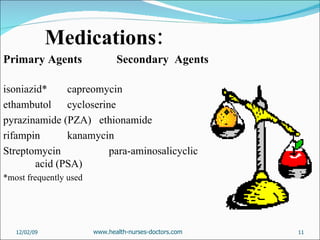
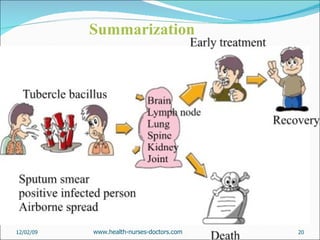



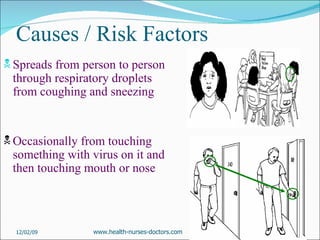
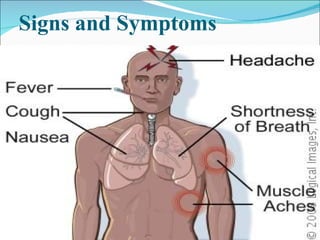

TB is caused by Mycobacterium tuberculosis bacteria affecting the lungs. It is spread through airborne droplets when infected people cough, sneeze or spit. Symptoms include cough, fever, weight loss and night sweats. Diagnosis involves tuberculin skin testing or sputum smear and culture. Treatment requires taking multiple antibiotics for 6-12 months.




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

