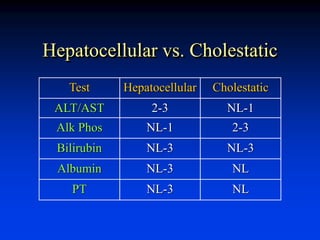
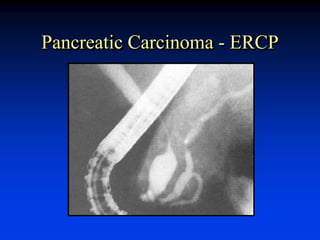
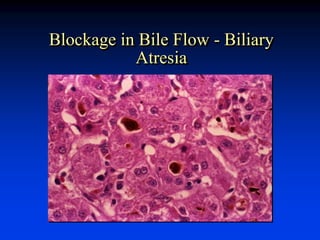
Liver function tests can evaluate for liver injury and dysfunction. Elevated levels of aminotransferases AST and ALT indicate hepatocyte injury, while elevated alkaline phosphatase and bilirubin suggest cholestasis or bile flow obstruction. Tests of synthetic function include albumin and coagulation factors. Specific diseases are identified by viral hepatitis serologies, iron studies, ceruloplasmin, and antimitochondrial antibodies. Abnormal tests must be interpreted in context of the clinical picture and potential non-hepatic causes. Liver biopsy may be needed to determine etiology and severity of injury when tests are inconclusive.



![Hepatic Metabolic Capacity
• Clearance must depend on total
functional mass or metabolic activity
• Hepatic drug metabolism -
[14C]amino-pyrine breath test
• Galactose elimination
• Not used clinically](https://image.slidesharecdn.com/20110722-czaja-lfts-230701043812-33b8eb7d/85/20110722-Czaja-LFTs-ppt-20-320.jpg)