LEARNING OBJECTIVES
• Introductionto LFTs
• Overview of functions of liver
• Liver function tests, enzymes, proteins & clotting factors which
are assessed in LFT, their normal values, and interpretation
• Bilirubin, its types and metabolism
• Symptoms of liver diseases
• Jaundice and its three types- Prehepatic, Hepatic and Post
Hepatic
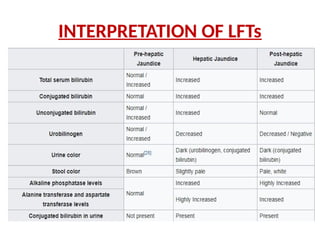
• Interpretation of LFT for each type of jaundice
• Estimation of bilirubin by kit method, reagents required,
procedure and calculation
3.
INTRODUCTION
• Liver FunctionTests (LFTs) is a group of tests that are performed
together to detect, evaluate, and monitor liver disease or damage
• LFTs measure enzymes, proteins, and substances that are
produced or excreted by the liver and are affected by liver injury.
Some are released by damaged liver cells and some reflect a
decrease in the liver's ability to perform one or more of its
functions.
• Liver function tests (include prothrombin time (PT/INR), activated
Partial ThromboplastinTime (aPTT), albumin, bilirubin (direct and
indirect), and liver enzymes (AST: Aspartate transaminase, ALT:
Alanine transaminase, ALP: Alkaline phosphatase and Gamma
Glutamyl transferase).
5.
What are liverfunction tests
• Liver function tests,also known as liver
chemistries,help determine the health of your
liver by measuring the level of proteins,liver
enzymes,and bilirubin in your blood.
6.
Why it's done
•To check for damage from liver infection's,such as
hepatitis B and hepatitis C.
• To monitor the side effects of certain medications
known to affect the liver.
• If you already have a liver disease,to monitor that
disease and how well a particular treatment is working.
• If you are experiencing the symptoms of a liver
disorder.
• If you have certain medical conditions such as
diabetes,high blood pressure, or anemia.
• If you drink alcohol heavily.
• If you have gallbladder disease.
7.
LIVER FUNCTION TESTS
1)BILIRUBIN
• Total bilirubin – measures all the yellow bilirubin pigment in the blood. Another test, direct
bilirubin, measures a form combined with another compound in the liver. Total Bilirubin
(conjugated and unconjugated): 0.1 to 1.2 mg/dL.
• Direct Bilirubin (conjugated): 0.1-0.4 mg/dL
• Indirect Bilirubin (unconjugated): 0.2-0.7 mg/dL
Aspect of liver function assessed: Indicator of the ability of the liver to conjugate and excrete
bilirubin.
Major utility: Aid in the differential diagnosis of jaundice
2) Alanine aminotransferase (ALT) – an enzyme mainly found in the liver. Normal level: 7 to 55
IU/L.
Aspect of liver function assessed: Serves as marker of injury to hepatocytes that contain ALT in
abundance
Major utility: The best test for detecting hepatitis. Early detector of liver damage
3) Aspartate aminotransferase (AST) – an enzyme found in the liver and a few other places,
particularly the heart and other muscles in the body. Normal levels: 8 to 48 IU/L
Aspect of liver function assessed: Serves as marker of injury to hepatocytes that contain AST in
abundance
Major utility: Early detector of liver damage
8.
LIVER FUNCTION TESTS
4)Alkaline phosphatase (ALP) – an enzyme related to the bile ducts.. Normal
level: 30-125 IU/L
Aspect of liver function assessed: Serves as marker of biliary obstruction
Major utility: Often increased when bile ducts are blocked
5)Gamma-glutamyl transferase (GGT) - an enzyme found mainly in the liver and is
a useful marker for detecting bile duct problems. Normal level: 6-50IU/L
6) PROTEINS:
• Albumin – measures the main protein made by the liver and tells whether or
not the liver is making an adequate amount of this protein. Normal Level 3.5-
5g/dL
• Total protein - measures albumin and all other proteins in blood,
including antibodies made to help fight off infections. Normal level: 6-8g/dL
• Albumin Globulin Ratio: Provides useful clinical information regarding
conditions such as hypoalbuminemia and multiple myeloma Normal range:
0.8-2:1
Aspect of liver function assessed: Measure of the biosynthetic function of the
liver, as the liver is the primary site of synthesis of most plasma proteins
Major utility: Indicator of severity of chronic liver disease
9.
LIVER FUNCTION TESTS
7)Prothrombin time:
Aspect of liver function assessed: Measure of the biosynthetic
function of the liver, as several coagulation factors are
synthesized in the liver
Major Utility: Indicator of severity of acute liver disease
8) Blood Ammonia: Normal level: 15 – 45mg/dL
Aspect of liver function assessed: Indicator of the ability of the
liver to detoxify ammonia
Major utility: Levels are elevated in cirrhosis of liver with portal
hypertension and in disorders of urea cycle
10.
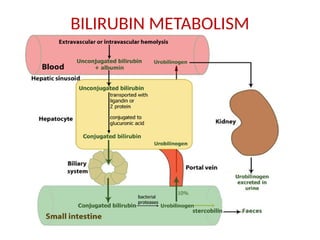
BILIRUBIN
• Bilirubin isbrownish yellow substance found
in bile. It is produced when the liver breaks
down old red blood cells. Bilirubin is then
removed from the body through urine as
urobilinogen and in the stool (feces) as
stercobilinogen which gives stool its normal
brown color.
11.
TYPES OF BILIRUBIN
•Unconjugated bilirubin(Indirect)
It is insoluble in water due to intermolecular hydrogen
bonding, it binds to albumin and travels through the
bloodstream to the liver.
•Conjugated bilirubin (direct)
Conjugated bilirubin is soluble in water and is made by
the liver from when unconjugated bilirubin conjugates
with glucuronic acid by the enzyme glucuronyltransferase.
.
SYMPTOMS OF LIVERDISEASES
• A variety of diseases and infections can cause acute or chronic damage to
the liver, causing inflammation, scarring, bile duct obstructions, clotting
abnormalities, and liver dysfunction. Alcohol, drugs, some herbal
supplements, and toxins can also pose a threat.
Symptoms of liver diseases are:
• Jaundice
• Dark urine
• Light-coloured stools,
• Nausea,
• Fatigue,
• Diarrhoea
• Edema and ascites, and
• Unexplained weight loss or gain emerge.
14.
JAUNDICE
• Jaundice isa condition in which the skin,
sclera of the eyes and mucous membranes
turn yellow because of a high level of bilirubin,
a yellow-orange bile pigment.
Types of jaundice:
• Prehepatic/Hemolytic
• Intrahepatic/Hepatocellular
• Post hepatic/Obstructive
15.
TYPES OF JAUNDICE
Prehepatic/Hemolytic:
Thepathology occurs prior to the liver metabolism, due to a pathological increased rate
of red blood cell (erythrocyte) hemolysis. The increased breakdown of erythrocytes
→ increased unconjugated serum bilirubin → increased deposition of unconjugated
bilirubin into mucosal tissue.
Total bilirubin: 0.3-1.0 mg/dL. jaundice may not be recognizable until levels are above
2.5 mg/dL.
There is an unconjugated hyperbilirubinemia in preheptic jaundice.
Causes:
• Sickle cell anemia
• Spherocytosis
• Thalassemia
• Glucose-6-phosphate dehydrogenase deficiency
• Microangiopathic hemolytic anemia
• Hemolytic-uremic syndrome
• Severe malaria (in endemic countries)
Symptoms:
Anemia and Jaundice. Apart form these symptoms, other symptoms are specific for each
condition.
17.
TYPES OF JAUNDICE
Intrahepatic/Hepatocellular:Caused by abnormal liver metabolism of bilirubin. The
pathology is due to significant damage to hepatocytes — due to infectious,
drug/medication-induced, auto-immune etiology. There is a reduced conjugation of
bilirubin by the damaged hepatocytes and a defective transport of conjugated
bilirubin to the biliary system. Therefore, there will be both unconjugated and
conjugated hyperbilirubiemia
Causes:
• Alcoholic liver disease
• Viral hepatitis: Hep A, B and C
• Iatrogenic, e.g. medication
• Hereditary haemochromatosis
• Autoimmune hepatitis
• Primary biliary cirrhosis or primary sclerosing cholangitis
• Hepatocellular carcinoma
• Cirrhosis
Symptoms: In addition to jaundice, following symptoms will be found in these
conditions:
• Itching of the skin, Nausea and vomiting, Abdominal pain, fever, weakness, dark
colored urine, edema and ascites
19.
TYPES OF JAUNDICE
Posthepatic/obstructive:The pathology occurs after bilirubin conjugation in the liver. Caused by a
blockage of bile ducts which transport bile containing conjugated bilirubin out of the liver for
excretion. Hence there is conjugated hyperbilirubinemia in obstructive jaundice.
Causes:
a) Intra hepatic Obstruction
• Biliary atresia (blockage of tube)
• Primary Biliary Cirrhosis
• Cirrhosis
• Malignant infiltration of ducts
b) Extra hepatic obstruction
• Gallstones, choledocholethiasis (stone in common bile duct)
• Cancer (pancreatic and gallbladder/bile duct carcinoma),
• Strictures of the bile ducts, (narrowing)
• Pressure on the common bile duct from enlarged lymph nodes
• Cholangitis (infection of the common bile duct
• Acute and chronic Pancreatitis
Symptoms: Jaundice, Fever, Weight loss, pale stools, Enlarged liver, Enlarged spleen, pruritis,
Edema, ascites
Note: Almost in all causes of hepatic and post hepatic jaundice, there is cholestasis. Cholestasis is a
condition the bile accumulates in the biliary tract when there is either decreased flow of bile due
to impaired secretion by the hepatocytes, or due to obstruction of bile through the bile ducts
ESTIMATION OF BILIRUBINBY KIT METHOD
OBJECT:
• To estimate Total and Direct Bilirubin by Kit method and Indirect Bilirubin by
deduction
PRINCIPLE:
• Bilirubin reacts with diazotized Sulfanilic acid (Sulfanilic acid and Sodium nitrite
in the ratio of 4:1) in the presence of an Accelerator (Caffeine, Sodium benzoate
and Sodium acetate ) to form an Azo dye which is red in neutral solution and
blue in alkaline solution (Fehling solution II containing Potassium sodium
tartrate and sodium hydroxide).
• The Total Bilirubin (indirect + direct) in blood is determined after the addition of
Accelerator because indirect Bilirubin reacts only in the presence of Accelerator.
Blue AzoBilirubin is formed in presence of alkaline Fehling solution which can be
measured by photometry using a 578nm filter.
• The water soluble conjugated Direct Bilirubin reacts directly without the need
for an Accelerator. Without the addition of alkali it forms a red Azo dye which
can be measured by photometry using a 546nm filter.
• The indirect Bilirubin can now be calculated from the difference between the
Total and Direct Bilirubin.
23.
ESTIMATION OF BILIRUBINBY KIT METHOD
• REAGENTS:-
R1 = Sulfanilic acid, R2 = Sodium Nitrite, R3 = Accelerator
(Caffeine, Sodium benzoate and Sodium acetate), R4 = Fehling
solution ll (potassium sodium tartrate and sodium hydroxide)
• SAMPLE:
Serum, heparinised or EDTA plasma are the preferred
samples.
Fresh samples should be taken
Avoid direct light exposure
Avoid hemolysis
24.
ESTIMATION OF BILIRUBINBY KIT METHOD
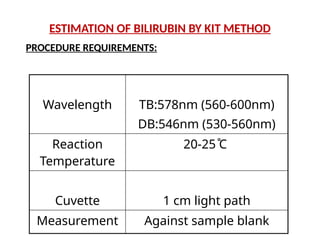
Wavelength TB:578nm (560-600nm)
DB:546nm (530-560nm)
Reaction
Temperature
20-25 ̊C
Cuvette 1 cm light path
Measurement Against sample blank
PROCEDURE REQUIREMENTS:
25.
ESTIMATION OF BILIRUBINBY KIT METHOD
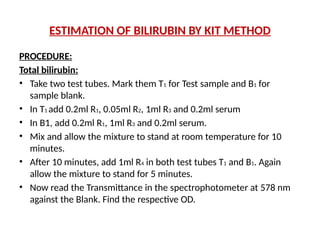
PROCEDURE:
Total bilirubin:
• Take two test tubes. Mark them T1 for Test sample and B1 for
sample blank.
• In T1 add 0.2ml R1, 0.05ml R2, 1ml R3 and 0.2ml serum
• In B1, add 0.2ml R1, 1ml R3 and 0.2ml serum.
• Mix and allow the mixture to stand at room temperature for 10
minutes.
• After 10 minutes, add 1ml R4 in both test tubes T1 and B1. Again
allow the mixture to stand for 5 minutes.
• Now read the Transmittance in the spectrophotometer at 578 nm
against the Blank. Find the respective OD.
26.
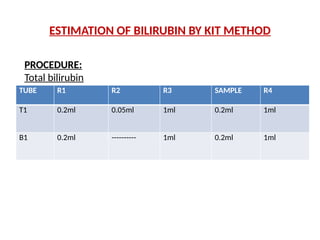
TUBE R1 R2R3 SAMPLE R4
T1 0.2ml 0.05ml 1ml 0.2ml 1ml
B1 0.2ml ---------- 1ml 0.2ml 1ml
PROCEDURE:
Total bilirubin
ESTIMATION OF BILIRUBIN BY KIT METHOD
27.
ESTIMATION OF BILIRUBINBY KIT METHOD
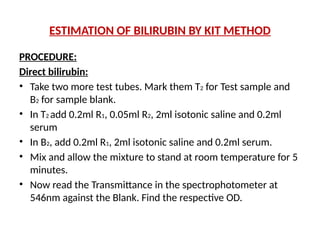
PROCEDURE:
Direct bilirubin:
• Take two more test tubes. Mark them T2 for Test sample and
B2 for sample blank.
• In T2 add 0.2ml R1, 0.05ml R2, 2ml isotonic saline and 0.2ml
serum
• In B2, add 0.2ml R1, 2ml isotonic saline and 0.2ml serum.
• Mix and allow the mixture to stand at room temperature for 5
minutes.
• Now read the Transmittance in the spectrophotometer at
546nm against the Blank. Find the respective OD.
28.
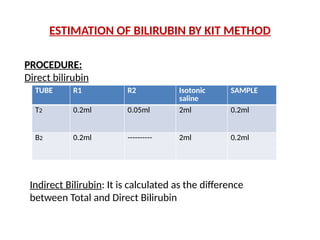
TUBE R1 R2Isotonic
saline
SAMPLE
T2 0.2ml 0.05ml 2ml 0.2ml
B2 0.2ml ---------- 2ml 0.2ml
PROCEDURE:
Direct bilirubin
Indirect Bilirubin: It is calculated as the difference
between Total and Direct Bilirubin
ESTIMATION OF BILIRUBIN BY KIT METHOD
29.
CALCULATIONS:-
• Multiply theOD of T1 and T2 with the Dilution
Factor given on the Kit
• Total Bilirubin = ODT1 X 10.5 mg/dl, Direct
Bilirubin = ODT2 X 14.0 mg/dl
• Indirect Bilirubin = Total - Direct
ESTIMATION OF BILIRUBIN BY KIT METHOD
30.
Result
• Total Bilirubin=...........mg/dl
• Direct Bilirubin= ..........mg/dl
.Indirect Bilirubin= .........mg/dl