Downloaded 183 times































The document provides an overview of lipids and lipoproteins. It defines lipids as biological compounds that are insoluble in water but soluble in organic solvents. The main classes of lipids are triglycerides, cholesterol, phospholipids and glycolipids. Lipids serve important functions like energy storage, cell membrane structure, and transport. The document discusses the structure and function of various lipoproteins involved in lipid transport, such as chylomicrons, VLDL, LDL, and HDL. It also covers lipid and lipoprotein measurement methods as well as their roles in health and disease.
Merlyn A. Baraclan presents an overview of lipids, including classifications and their role in metabolism.
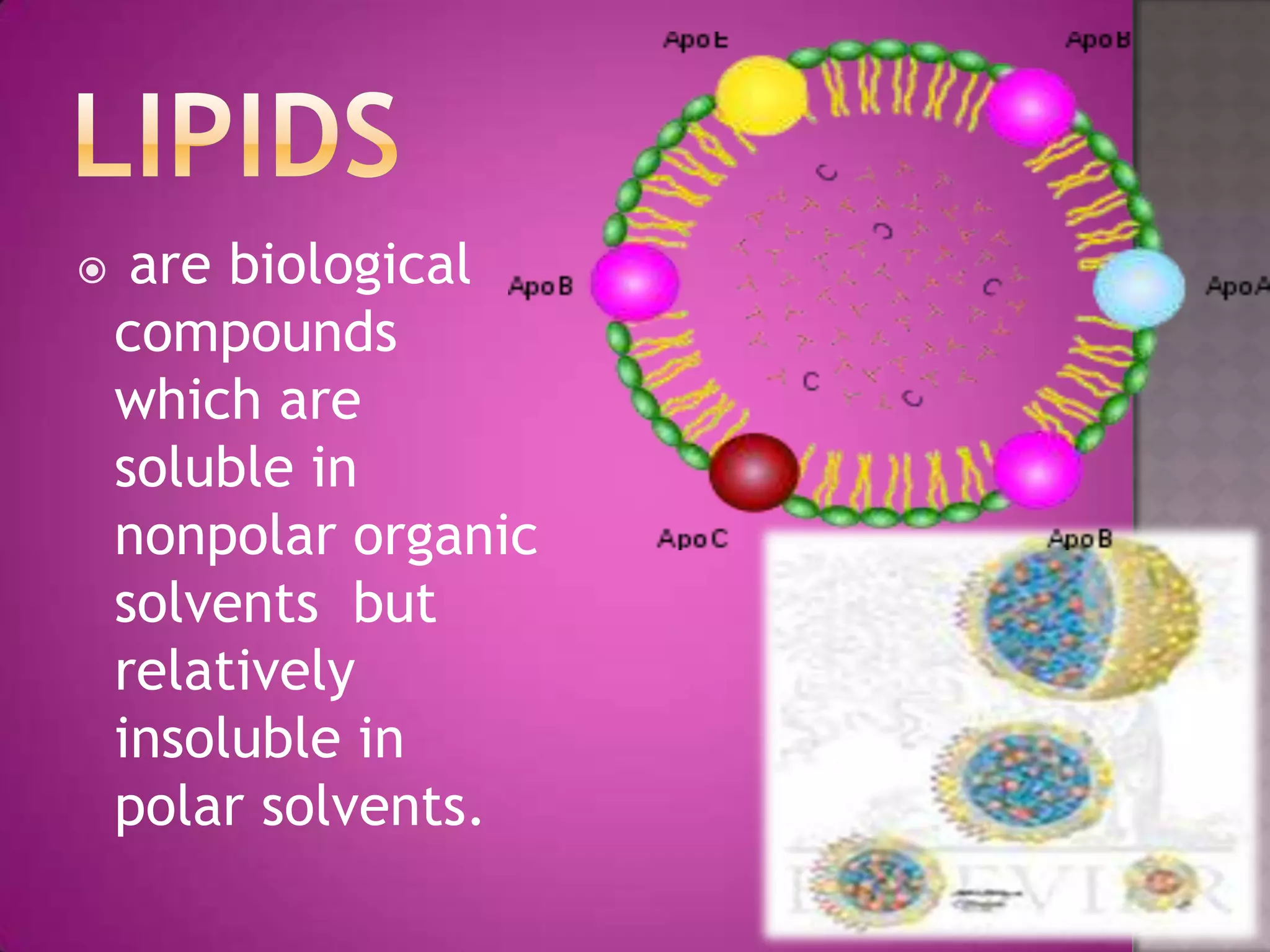
Lipids, soluble in nonpolar solvents, include triglycerides, cholesterol, and phospholipids, serving as fuel and structural components.
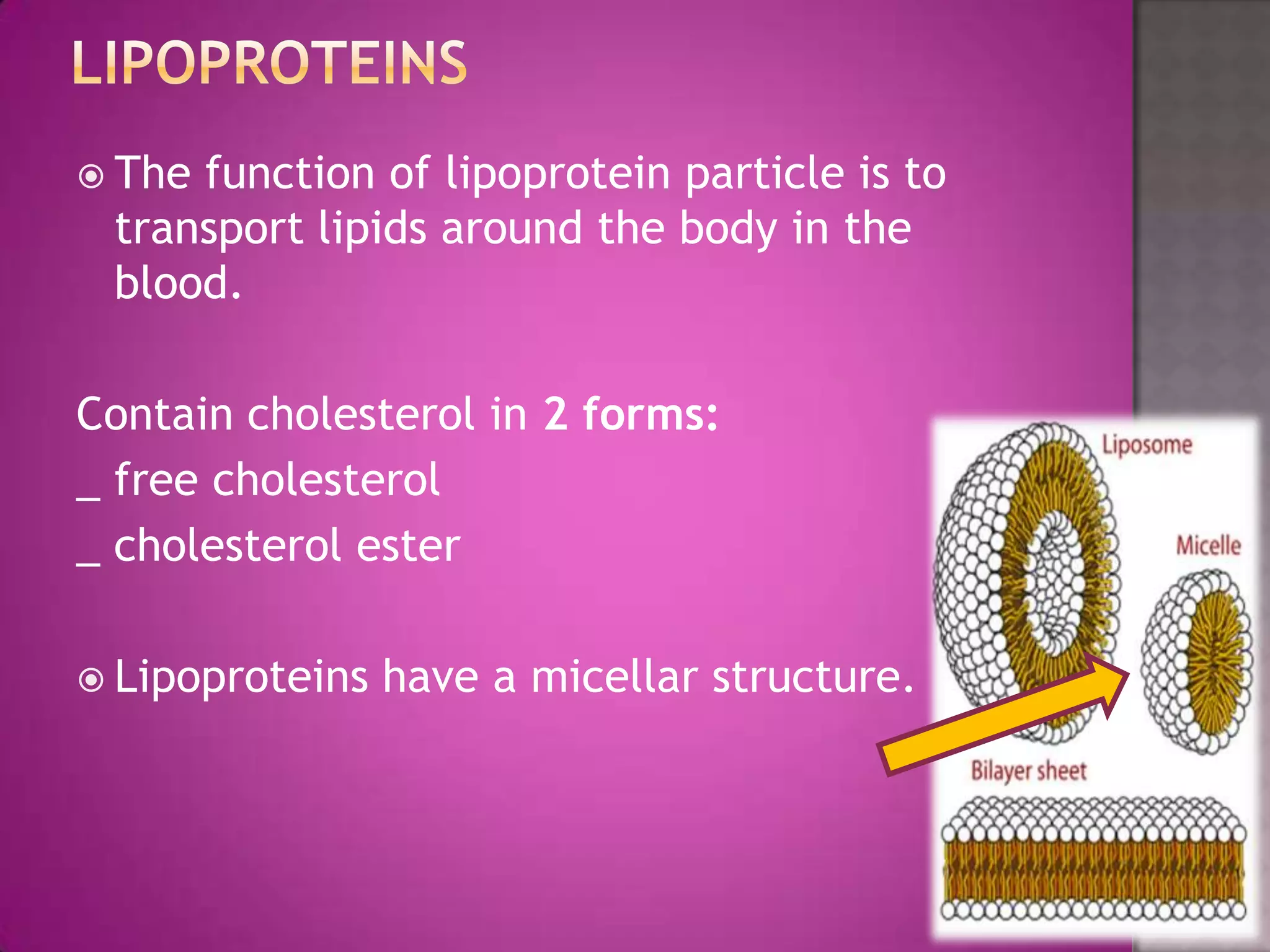
Lipoproteins transport lipids in blood, consisting of a central core of TAG/cholesterol and a surface coat of phospholipids and apolipoproteins.
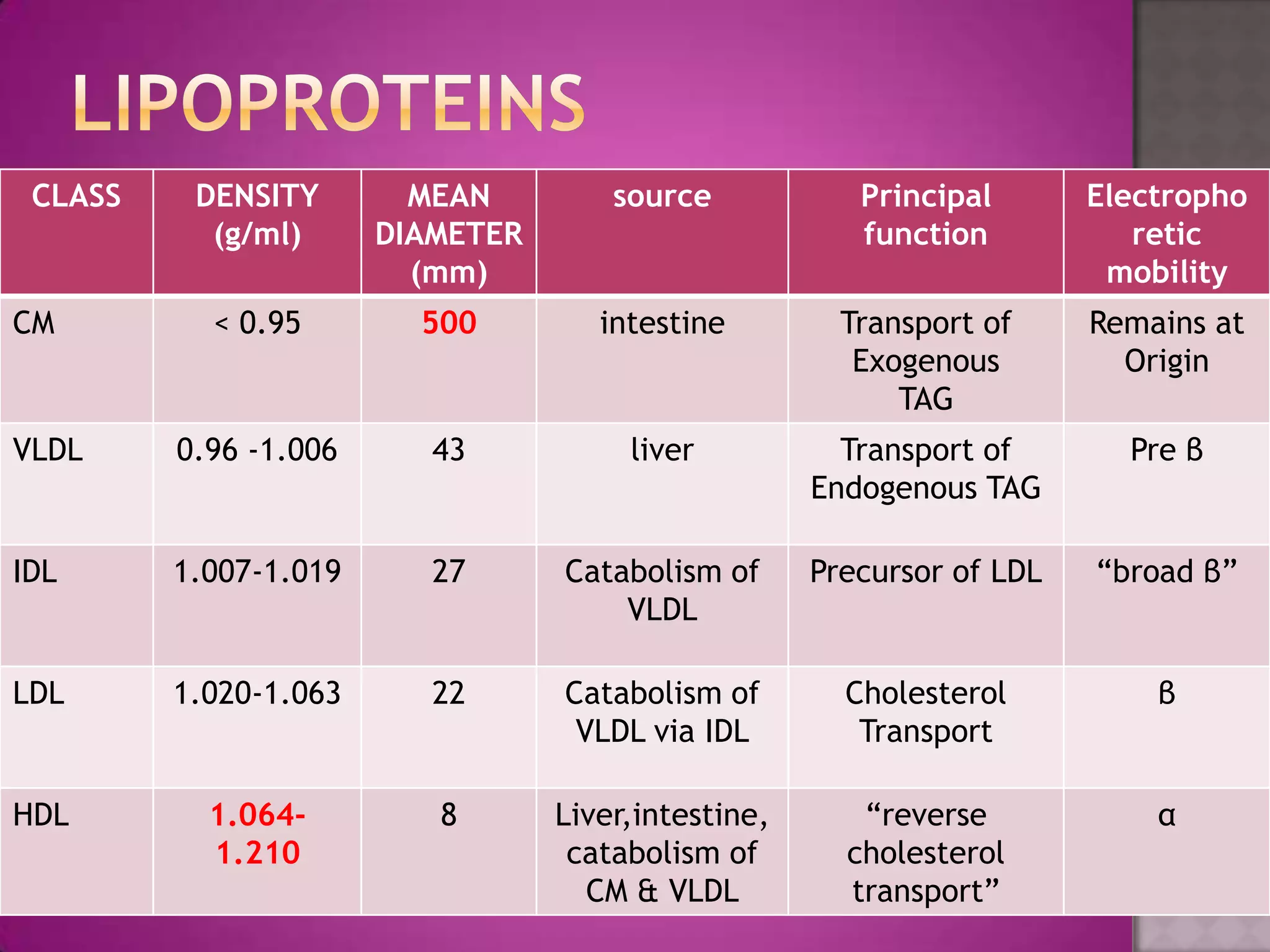
Categories of lipoproteins are defined by density, diameter, source, and functions, with a focus on TAG and cholesterol content.
Chylomicrons, VLDL, LDL, HDL—each with unique origins, lipid compositions, and physiological roles in lipid transport.
Discusses specific lipoprotein variants (Lp(a), LPX) and their clinical relevance in lipid metabolism.
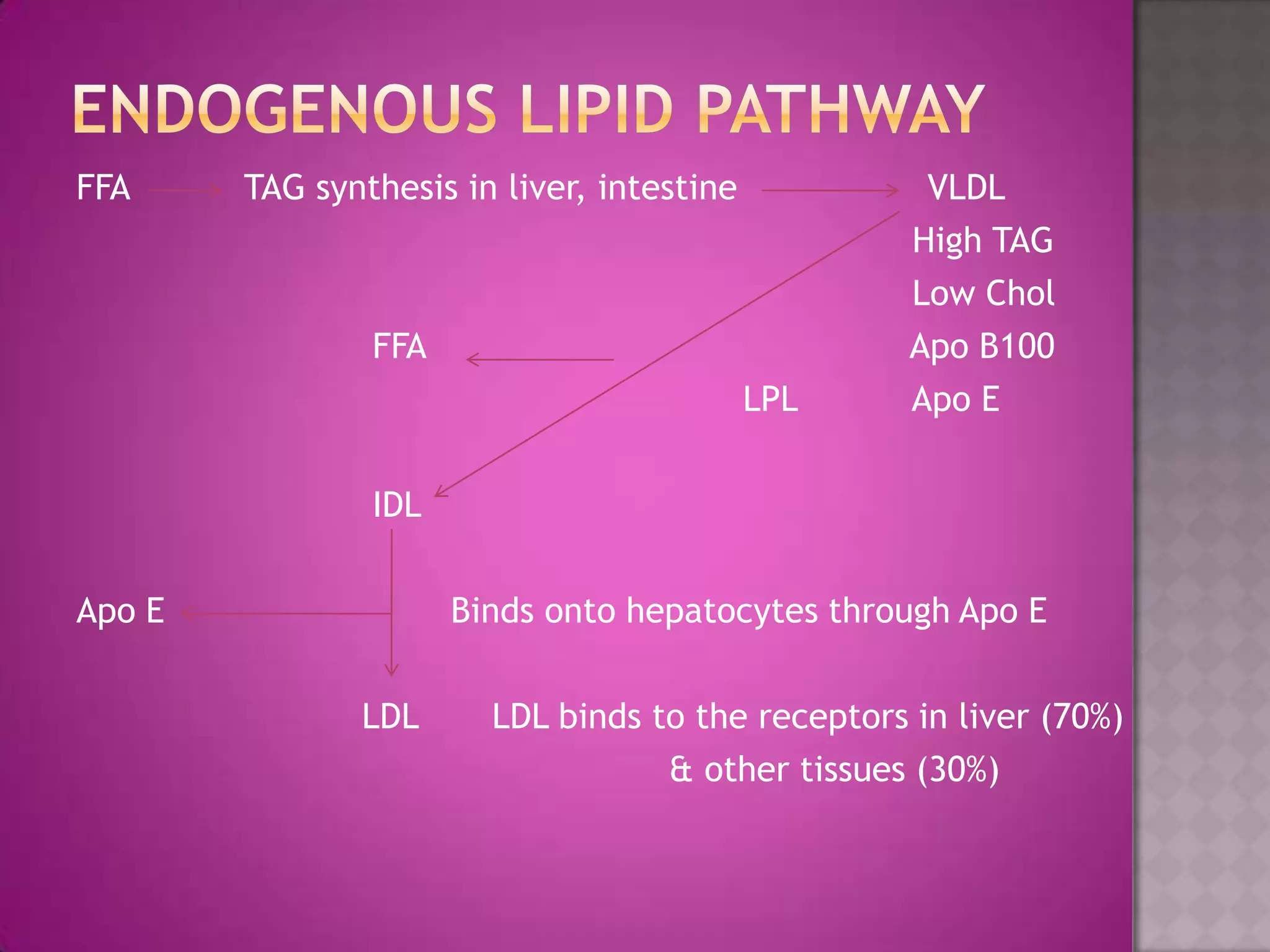
Mechanisms of TAG transport and cholesterol metabolism by various lipoproteins detailing their conversion and uptake by the liver.
Factors affecting lipid levels include biological variation, need for fasting, and distinctions between plasma and serum.
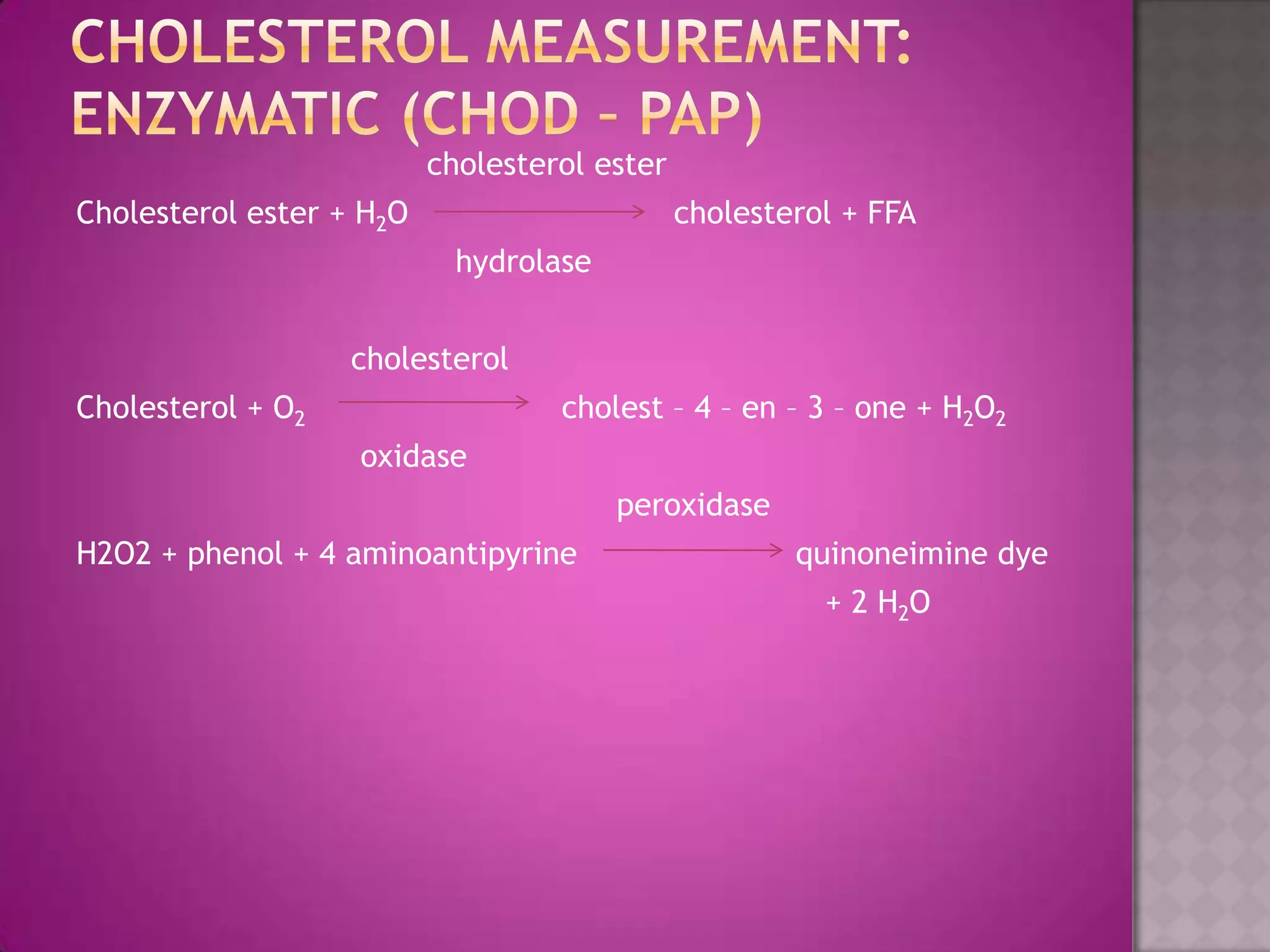
Methods for triglyceride and cholesterol measurement, including enzymatic and chemical techniques.
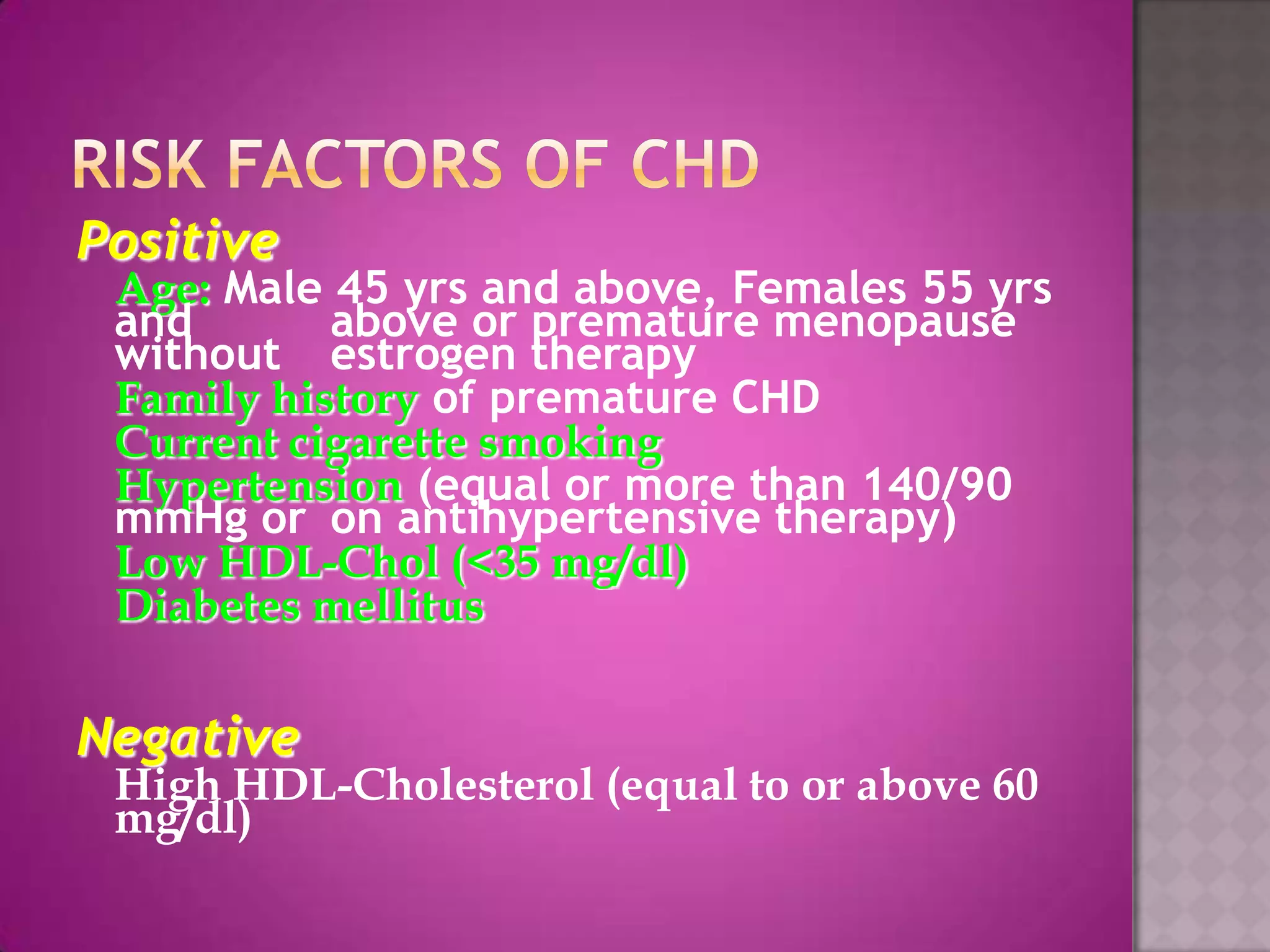
Cholesterol testing recommendations for adults, treatment goals, and lipid level classifications.
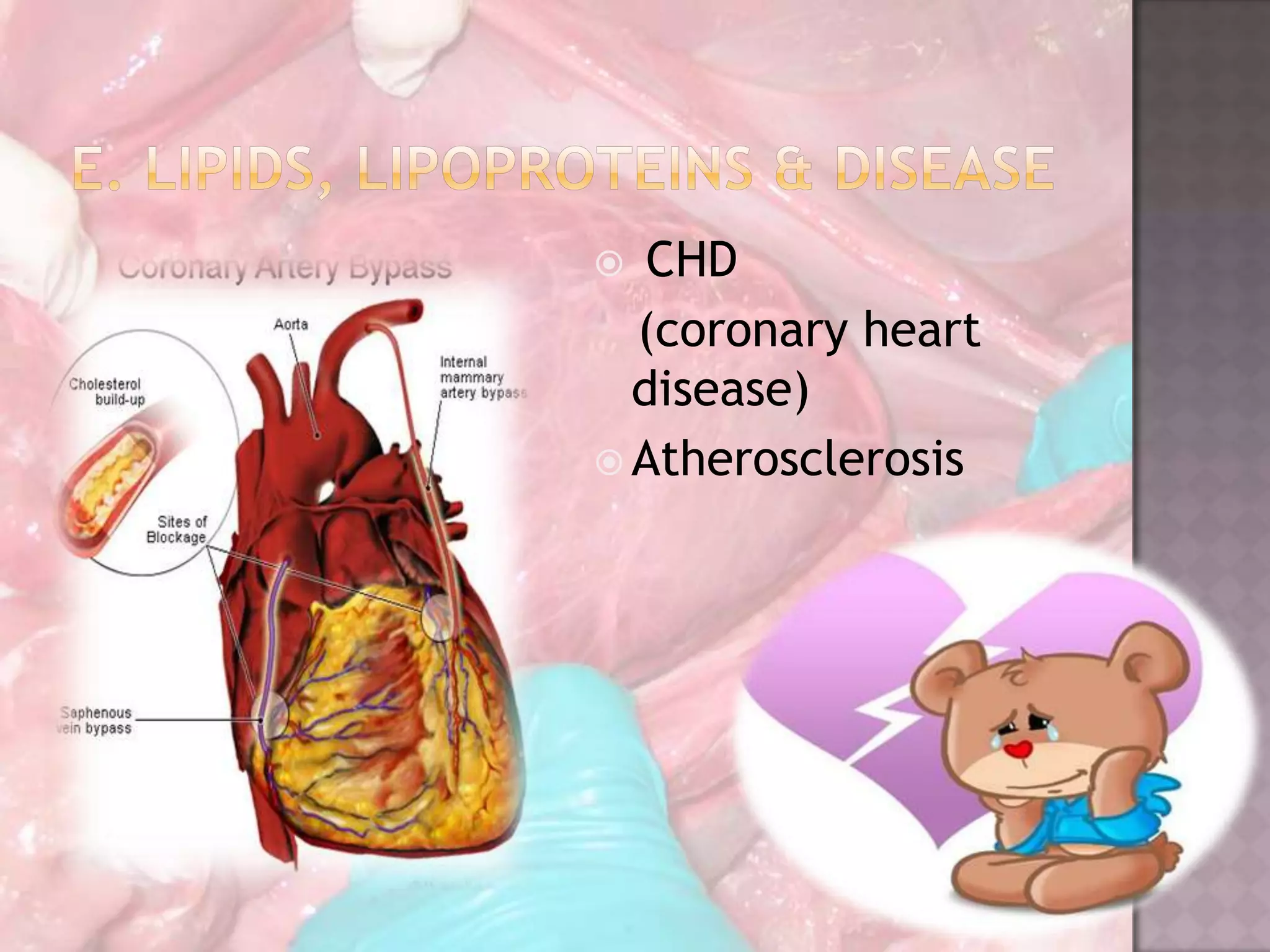
Common dyslipidemias associated with high LDL-C, TAG-rich particles, and genetic lipid storage disorders.
Historical significance of testing methods, current practices for assessing lipid profiles, and resources for further learning.











































































































