Downloaded 33 times

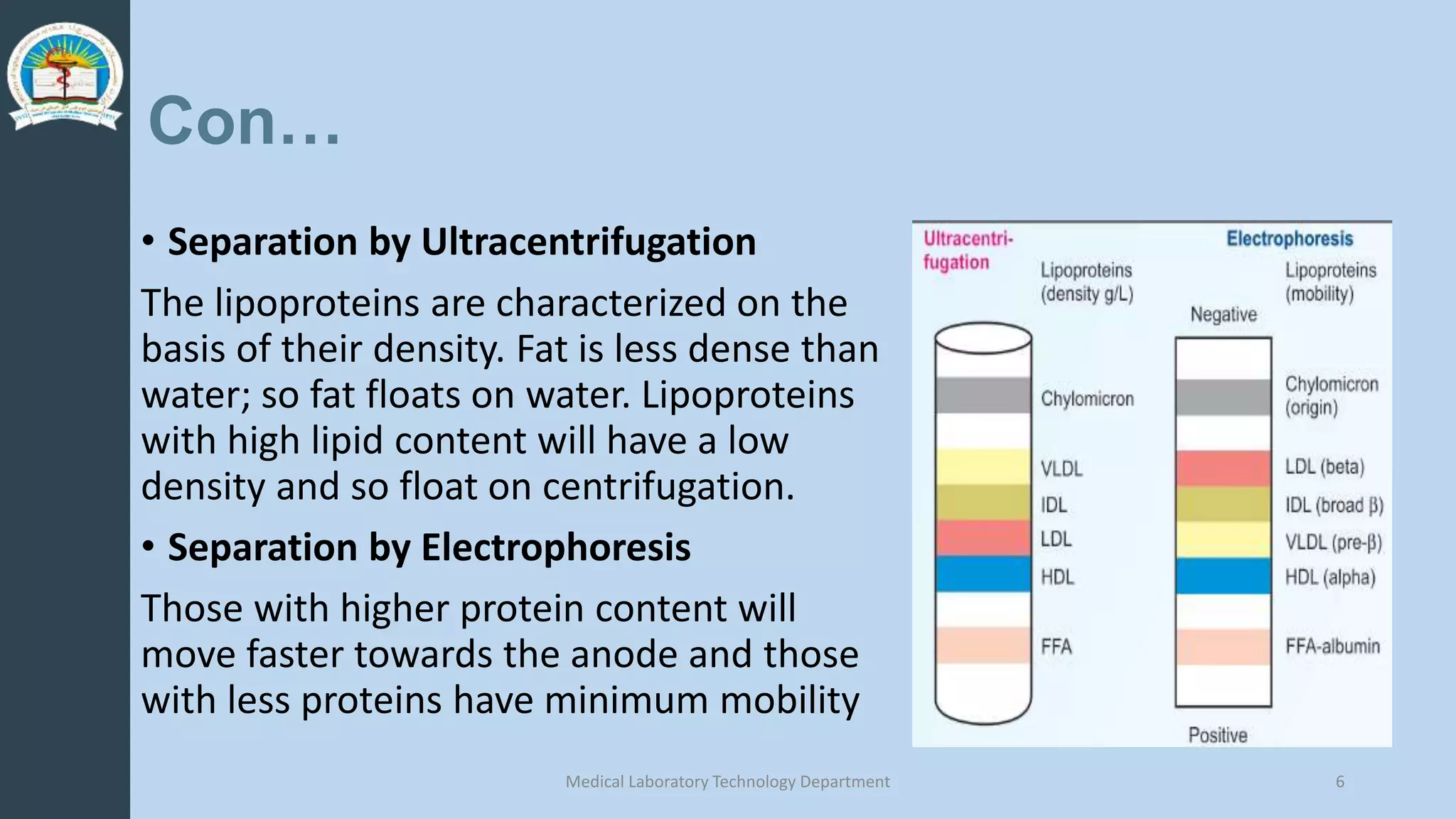
![Composition of lipoproteins
• Lipoproteins are composed of a neutral lipid core (containing
triacylglycerol [TAG] and cholesteryl esters) surrounded by a shell of
amphipathic apolipoproteins , phospholipid, and unesterified (free)
cholesterol
• These amphipathic compounds are oriented so that
their polar portions are exposed on the surface of
the lipoprotein, thereby rendering the particle soluble
in aqueous solution
Medical Laboratory Technology Department 4](https://image.slidesharecdn.com/conferancelipoproteins2-220509132834-94d5b6f0/75/Lipoprotein-Metabolism-pptx-4-2048.jpg)








![Metabolism of HDL
• HDL particles are formed in blood by the addition of lipid to apo A-1, an
apolipoprotein made by the liver and intestine and secreted into blood.
[HDLs are also formed within the liver and intestine.]
• HDL functions:
• Apolipoprotein supply:: Apo CII & apo E
• Uptake of unesterified cholesterol: Nascent HDL which is disk shaped particles take
up cholesterols from peripheral tissue.
• Esterification of cholesterol: cholestereol esterify to colesterol esters by LCAT.
Incresead cholesterol esters convert discoidal nascent HDL to spherical HDL3 and
HDL2. CETP moves some of cholestryl esters to VLDL in exchange for TAG.
• Reverse cholesterol transport: HDL transfer cholestrol from peripheral tissue to liver.
HDL is taken up by hepatic scavenger receptor B1. Hepatic lipase hydrolyzes HDL
phospholipid and TAG, and cholesterol esters are released into liver cells. The
cholesterol that reaches the liver is used for synthesis of bile acids or excreted as
such in bile. Therefor, HDL is called good cholesterol.
17](https://image.slidesharecdn.com/conferancelipoproteins2-220509132834-94d5b6f0/75/Lipoprotein-Metabolism-pptx-17-2048.jpg)


![Lipoprotein a or Lp (a)
• Lp (a) is structurally releated to LDL because both lipoproteins
possess one molecule of apo B-100 per particle with similar lipid
compositions. Unlike LDL, Lp(a) also contains a carbohydrate-rich
protein [apo(a)], which is covalently bound to the apo B-100 through
a disulfide linkage.
• Apo(a) is structurally homologous to plasminogen, the precursor of a
blood protease whose target is fibrin, the main protein component of
blood clots.
• It is hypothesized that elevated Lp(a) slows the breakdown of blood
clots that trigger heart attacks because it competes with plasminogen
for binding to fibrin.
20](https://image.slidesharecdn.com/conferancelipoproteins2-220509132834-94d5b6f0/75/Lipoprotein-Metabolism-pptx-20-2048.jpg)

![Reference
• Lippincott’s illustrated Reviews Biochemistry/[edited by] Denise R.
Ferrier- 6th edition
• Textbook of Biochemistry for Medical Students/[edited by] DM
Vasudevan, Sreekumari S, Kannan Vaidyanathan- 7th ed.
• Clinical chemistry : principles, techniques, and correlations/[edited by]
Michael L. Bishop, Edward P. Fody, Larry E. Schoeff.—8th ed.
• TIETZ FUNDAMENTALS OF CLINICAL CHEMISTRY/[edited by] Carl A.
Burtis, David E. Bruns- 7th edition
Medical Laboratory Technology Department 22](https://image.slidesharecdn.com/conferancelipoproteins2-220509132834-94d5b6f0/75/Lipoprotein-Metabolism-pptx-22-2048.jpg)


The document discusses lipoprotein metabolism, emphasizing their composition, classification, and various metabolic pathways, including chylomicrons, VLDL, LDL, and HDL. It outlines the roles of apolipoproteins and their functions in lipid transport and regulation, as well as the implications of lipoprotein levels on cardiovascular health. Additionally, it highlights the significance of HDL as 'good cholesterol' and its protective effects against heart disease.












































![Lipoprotein metabolism and CAD[1].pptx..](https://cdn.slidesharecdn.com/ss_thumbnails/lipoproteinmetabolismandcad1-250223181828-e4e0a658-thumbnail.jpg?width=640&height=640&fit=bounds)





























