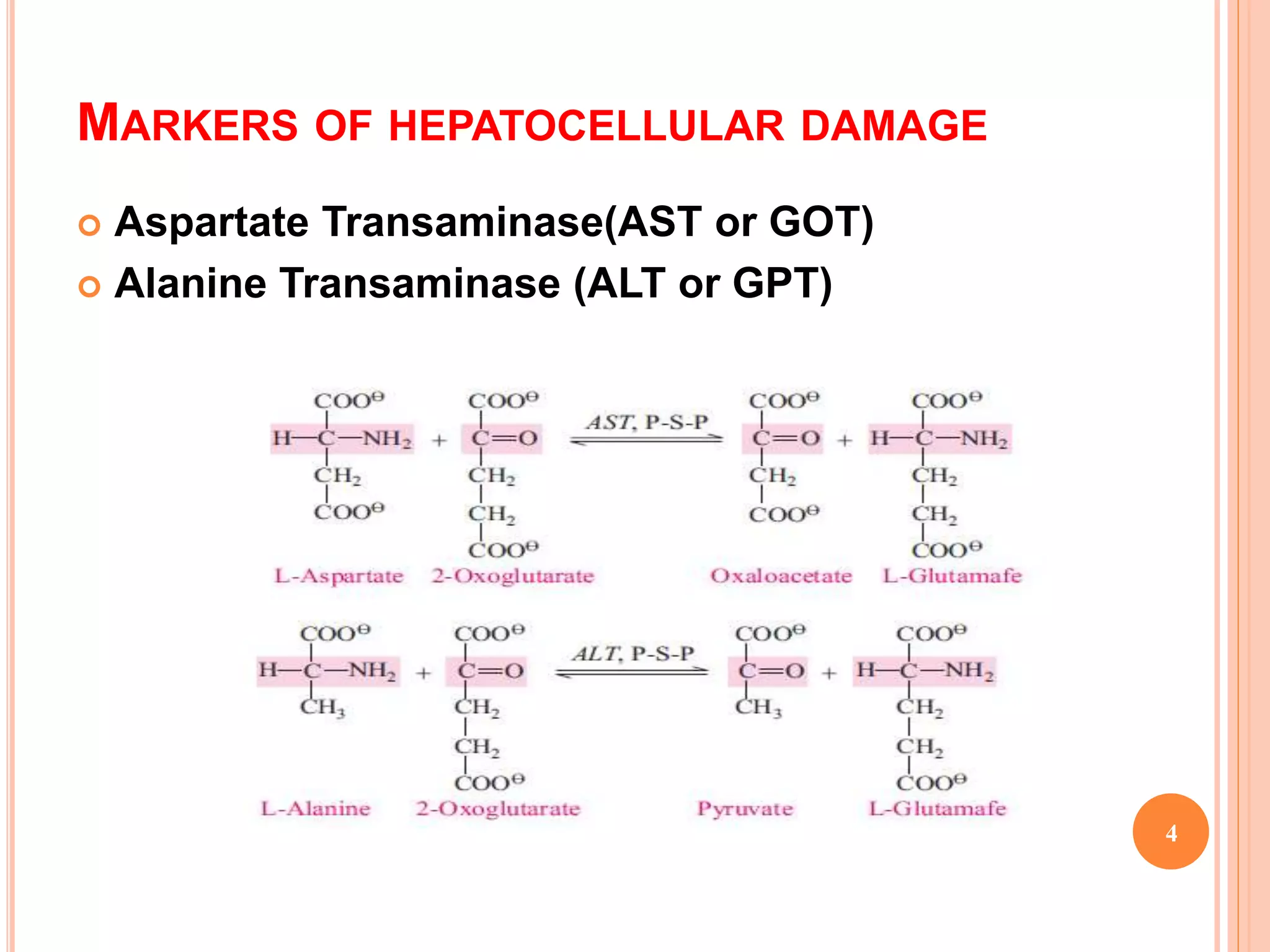
This document discusses serum enzymes that can indicate liver disease states. It outlines enzymes that reflect hepatocyte damage like ALT and AST, as well as enzymes that indicate cholestasis such as alkaline phosphatase, GGT, and 5'-nucleotidase. ALT and AST are more specific to liver injury than other tissues. Alkaline phosphatase is also elevated in bone diseases. GGT and 5'-nucleotidase are more sensitive markers of cholestasis than alkaline phosphatase. The document also presents two case studies, one with signs of alcoholic liver disease and another with possible liver metastases from lung cancer.