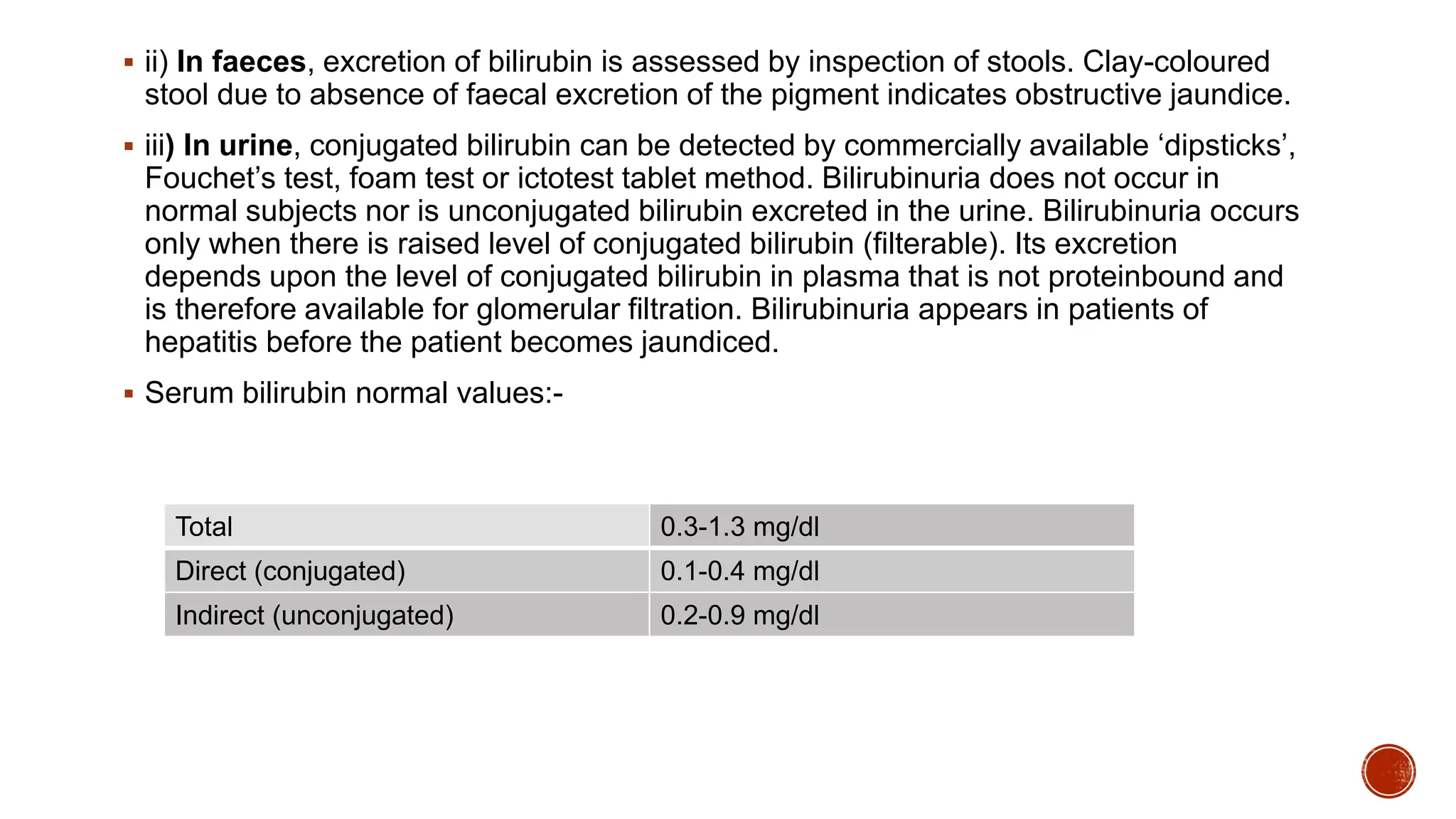
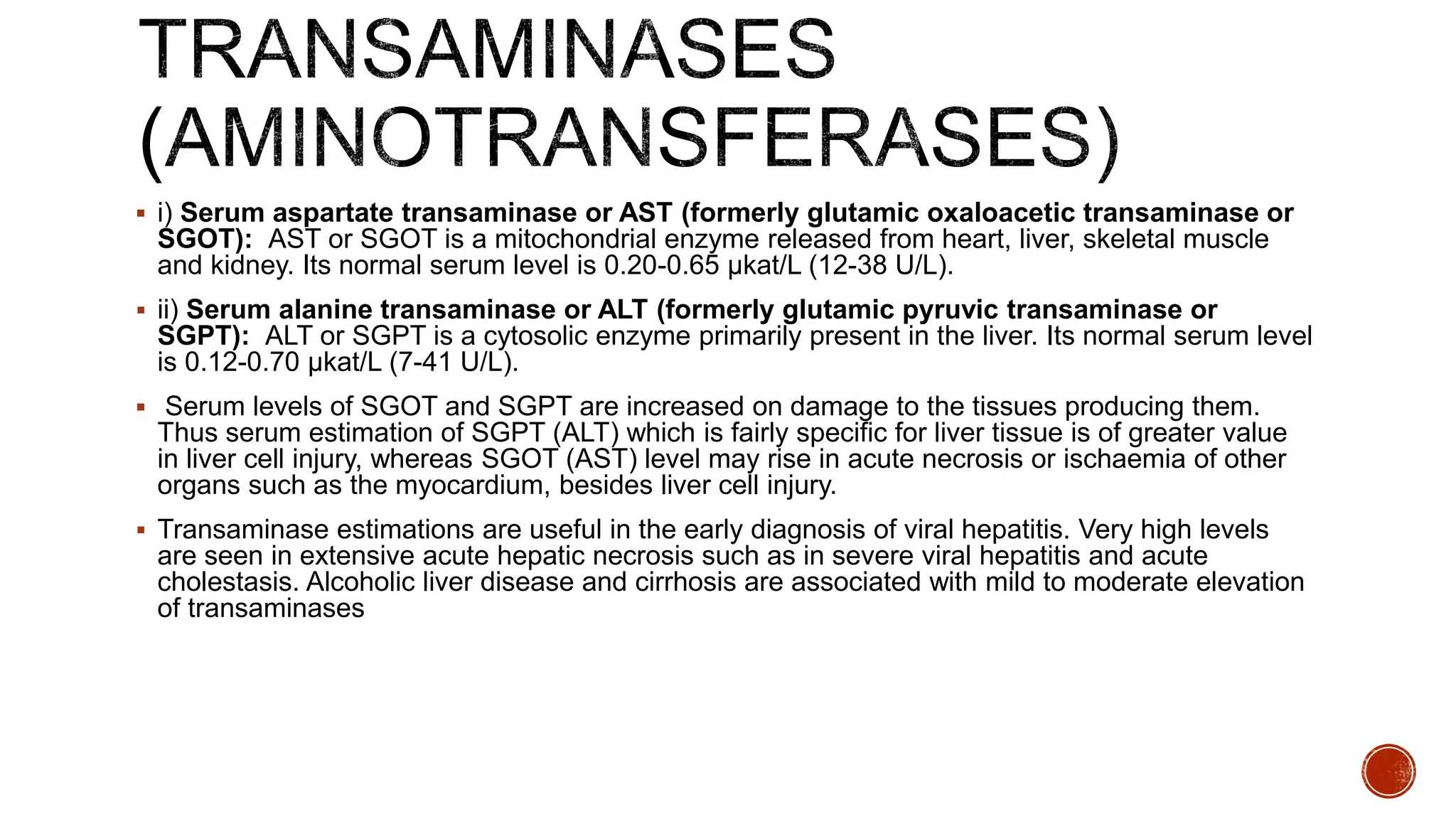
The document discusses liver function tests (LFTs). It begins by providing an overview of liver anatomy and physiology. It then discusses the various functions of the liver including metabolic, excretory, protective, hematological, and storage functions. The goals of LFTs are outlined as detecting liver disease, distinguishing disease types, and monitoring treatment response. Common LFTs are described such as bilirubin, alkaline phosphatase, GGT, AST, ALT, albumin, and prothrombin time. Elevations in these enzymes and proteins can indicate liver damage or disease. Causes and interpretations of abnormal LFT results are provided.