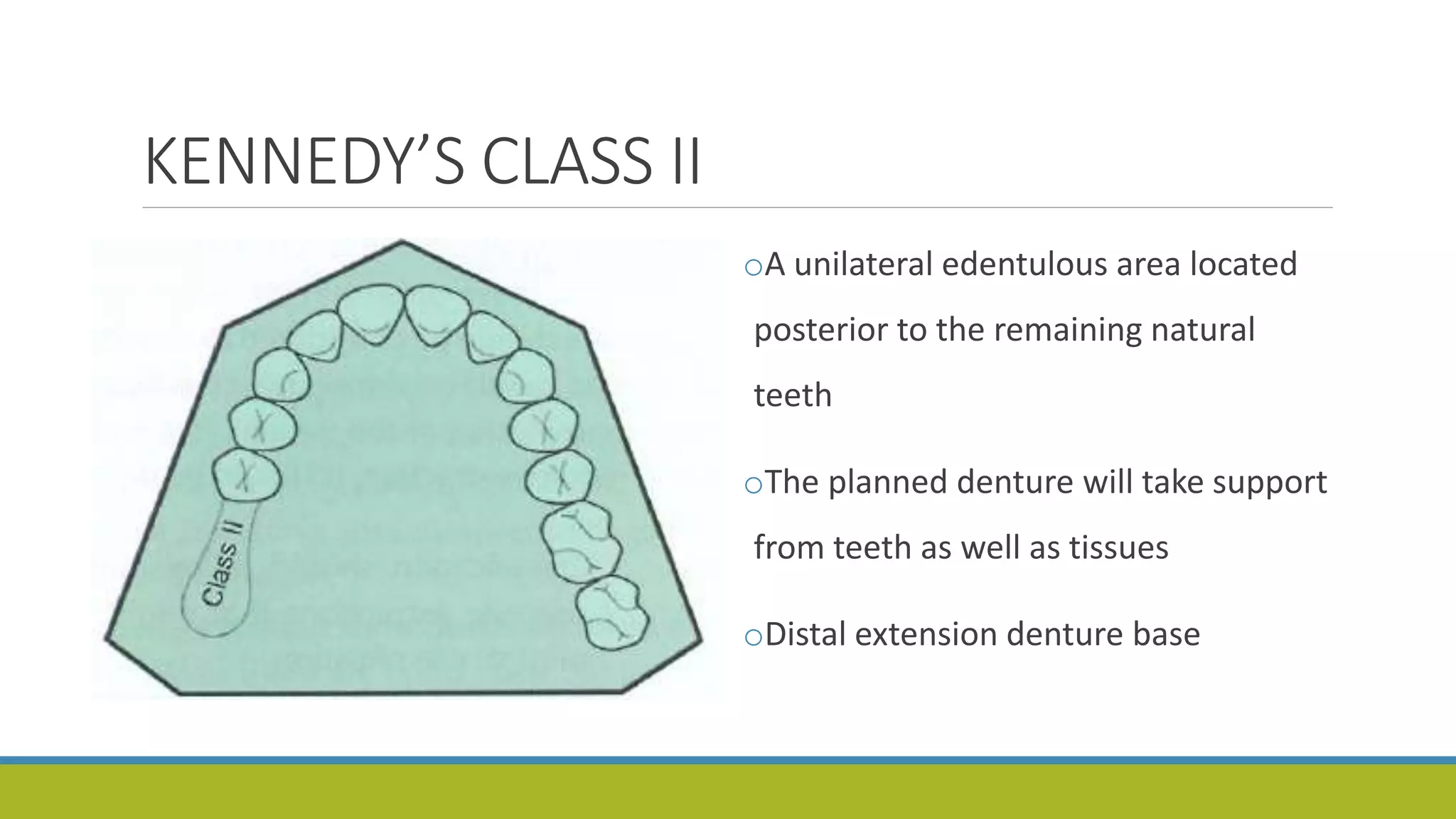
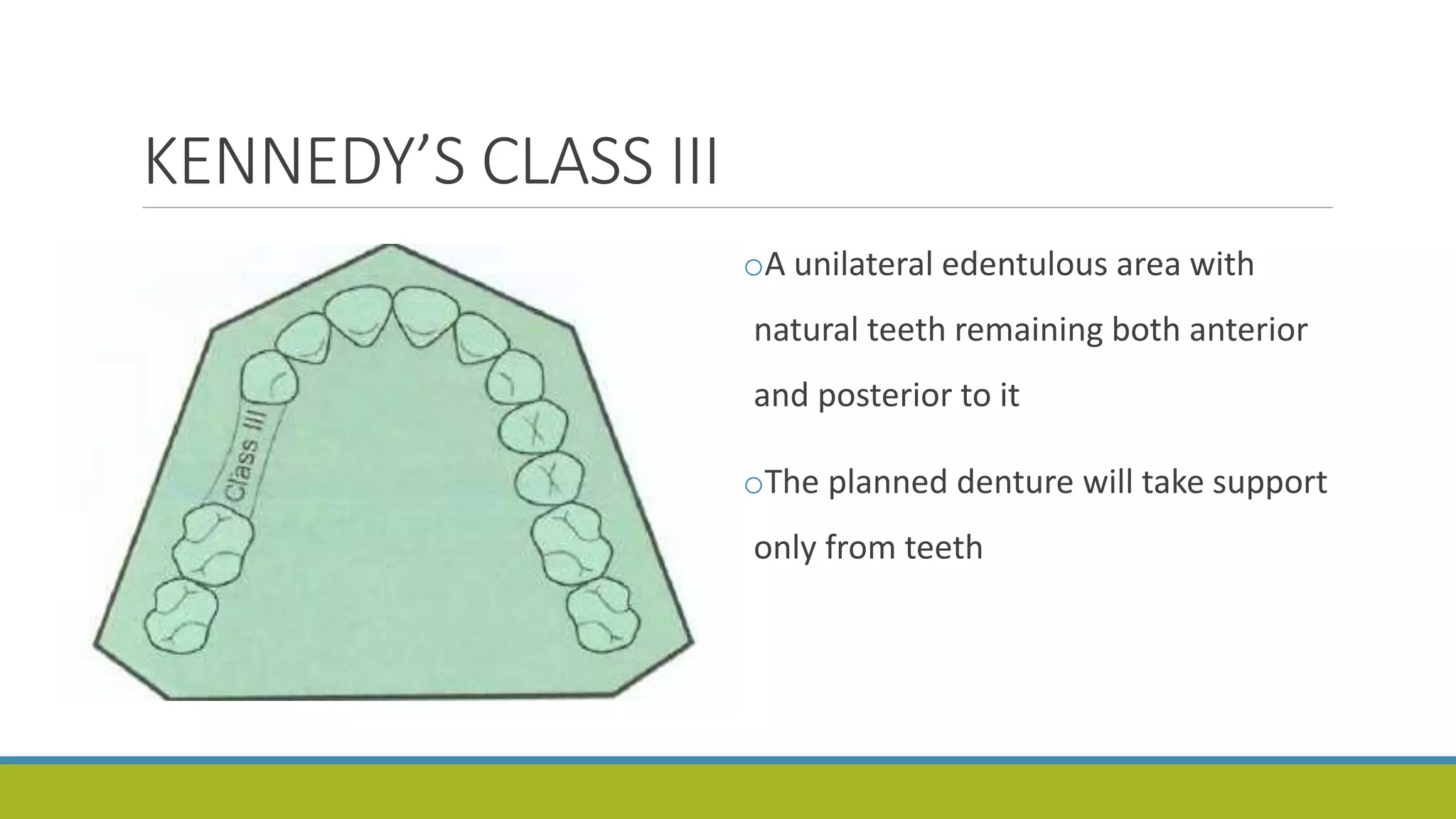
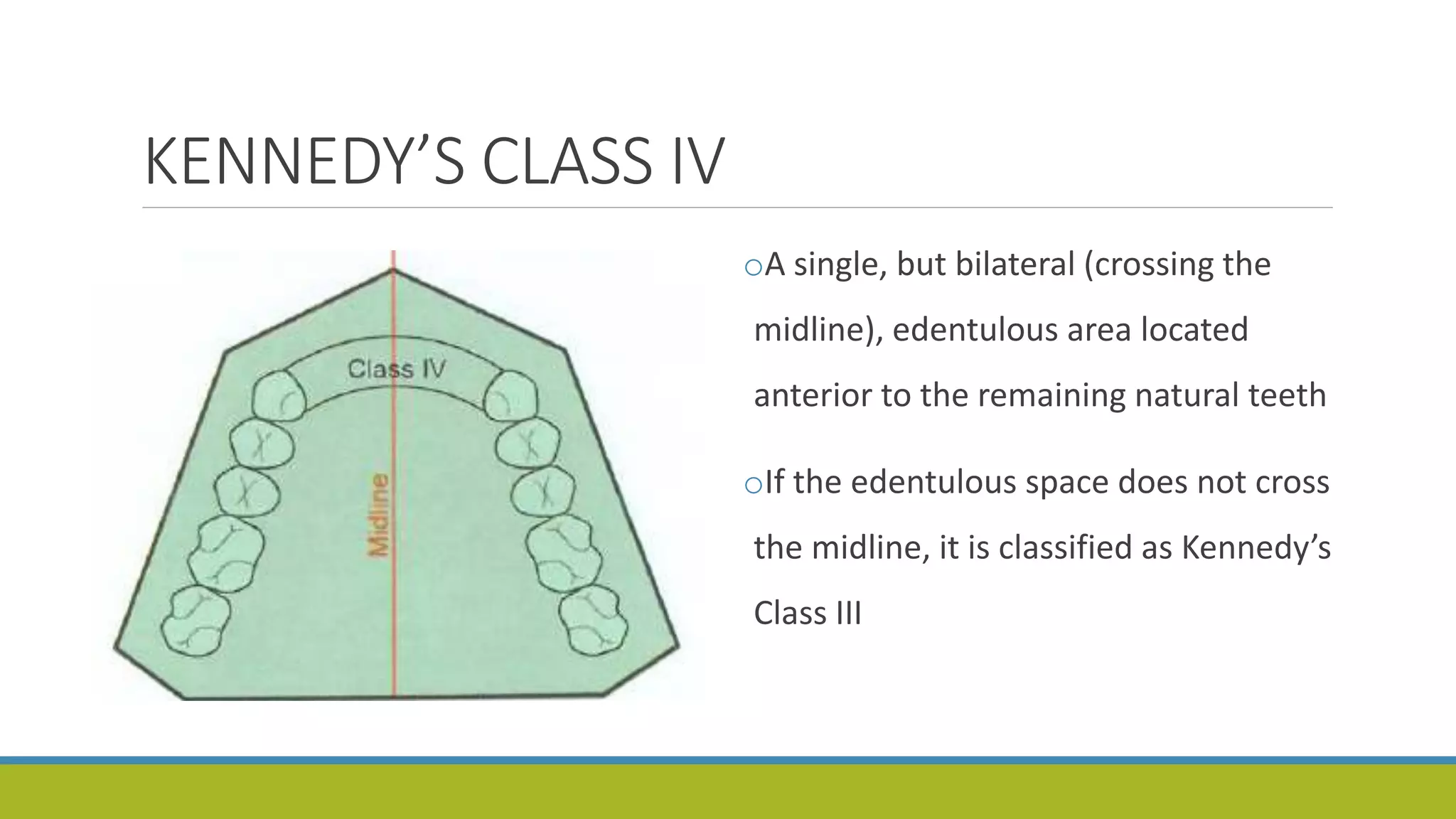
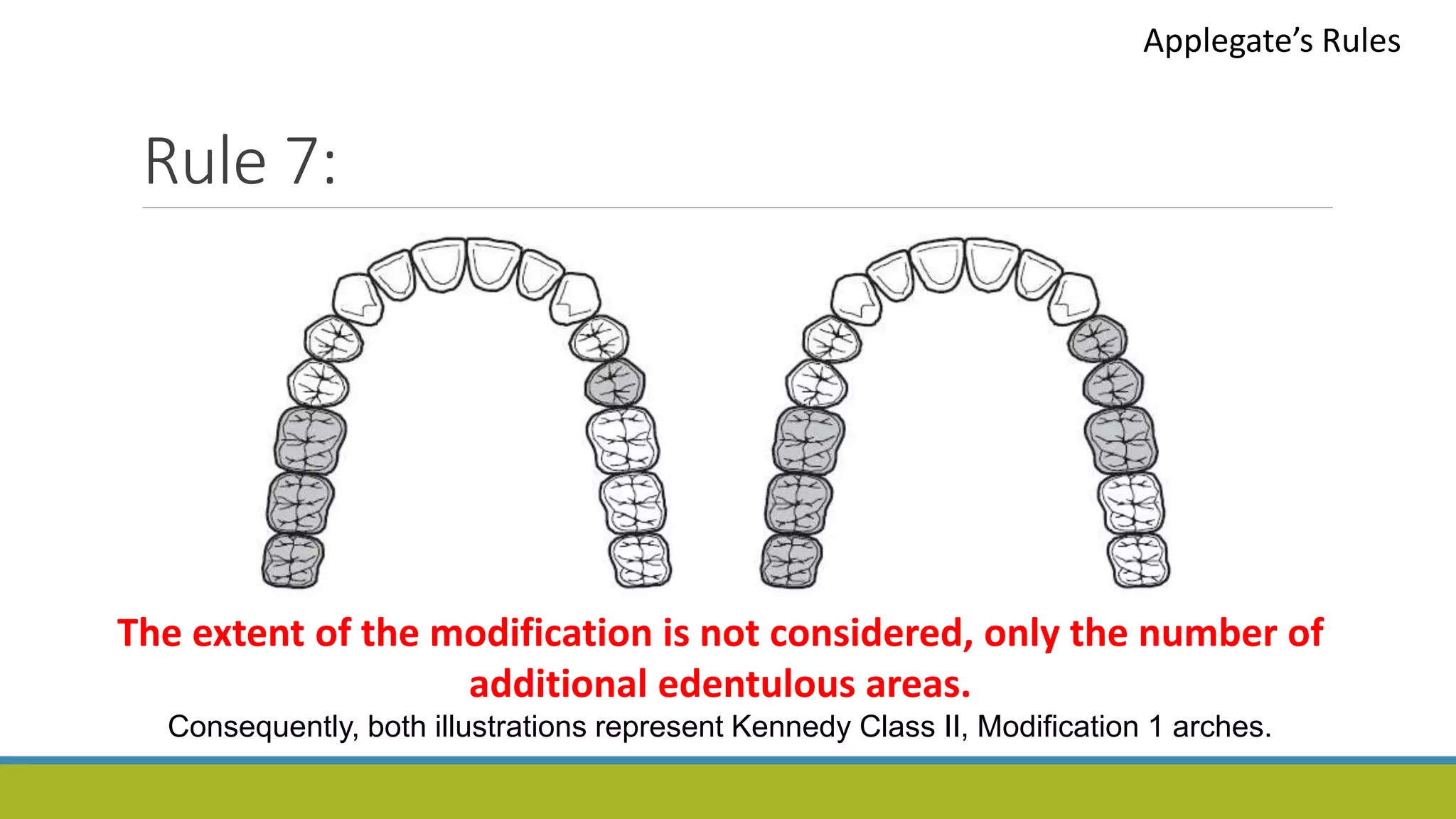
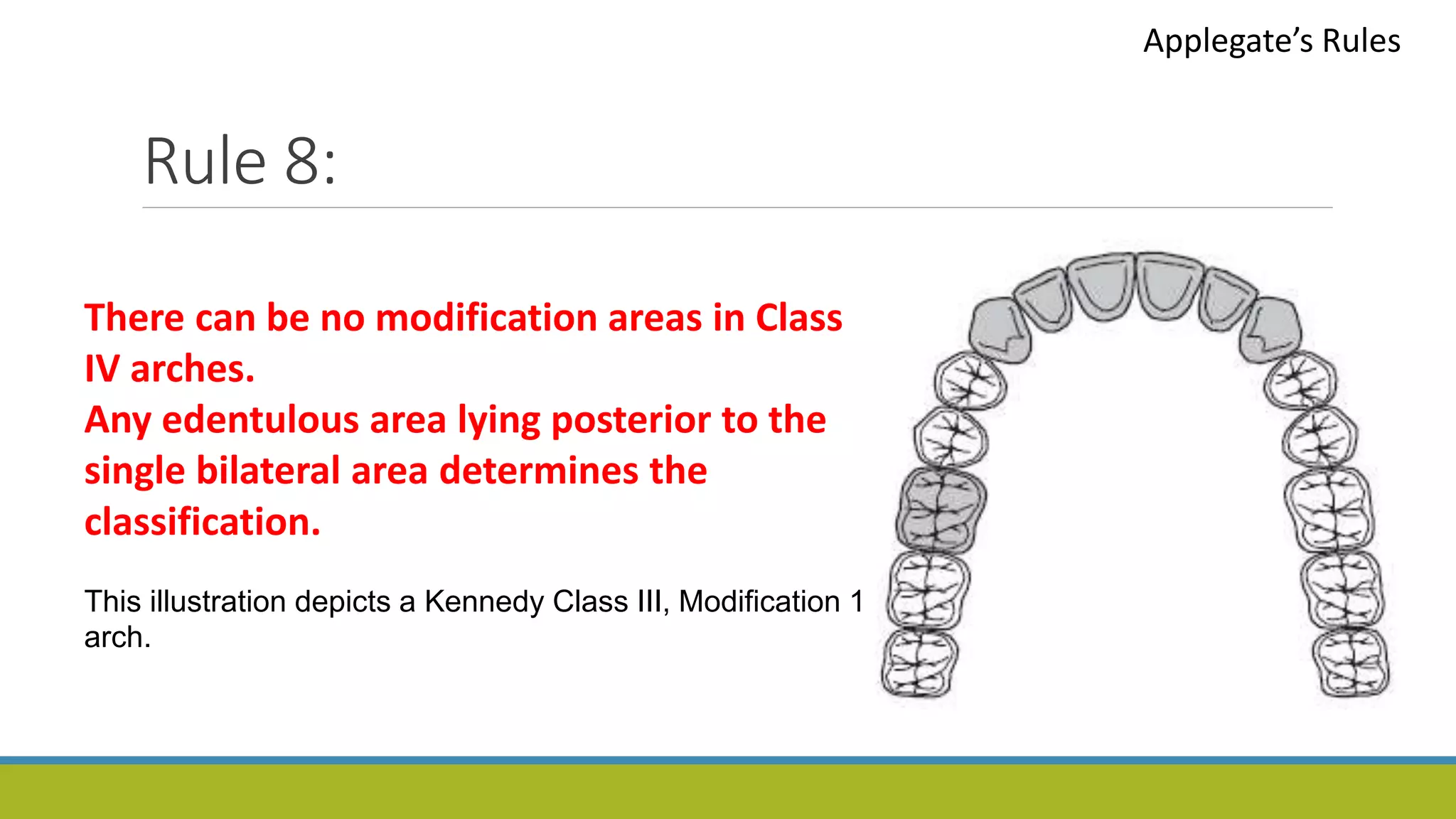
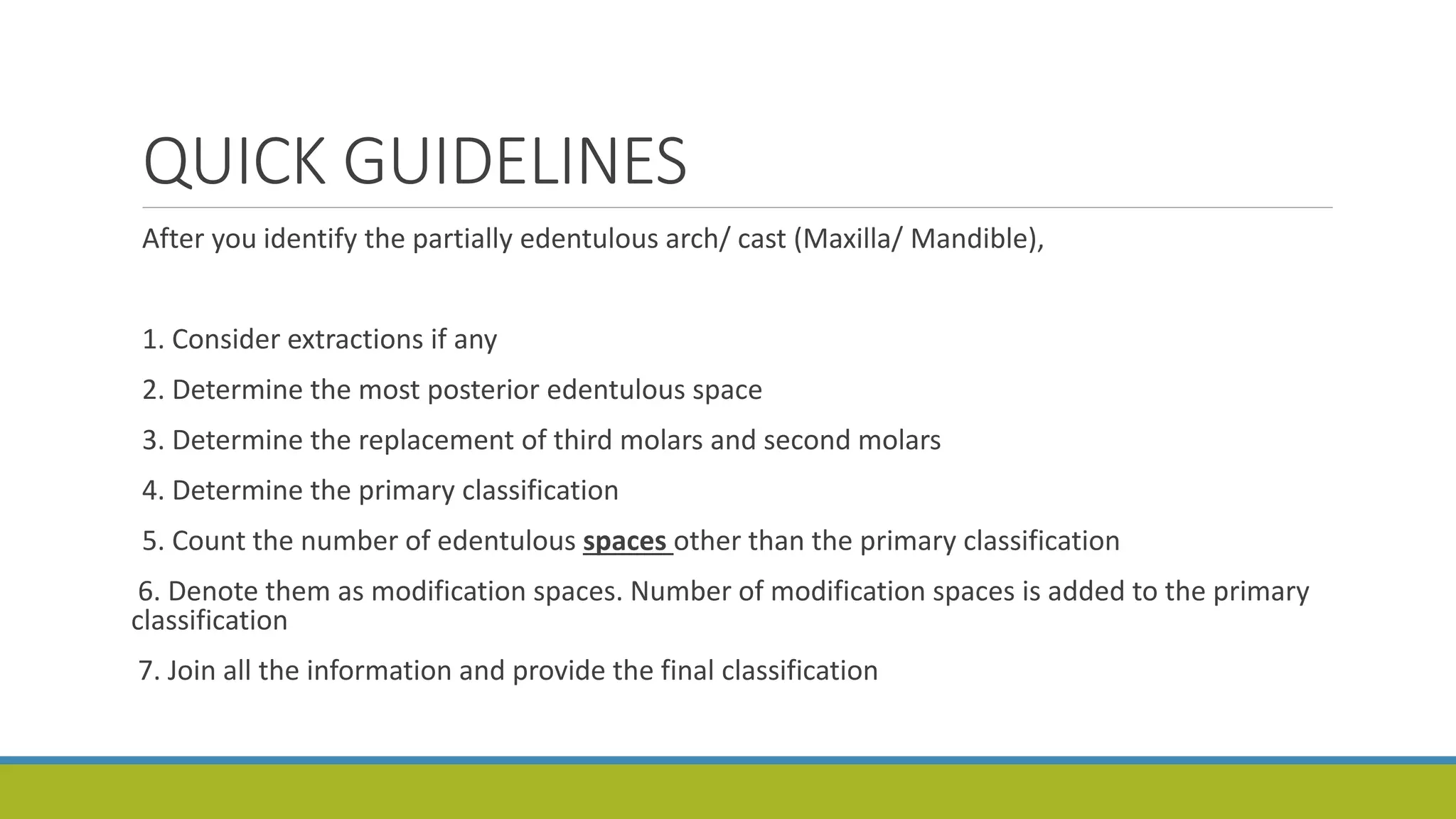
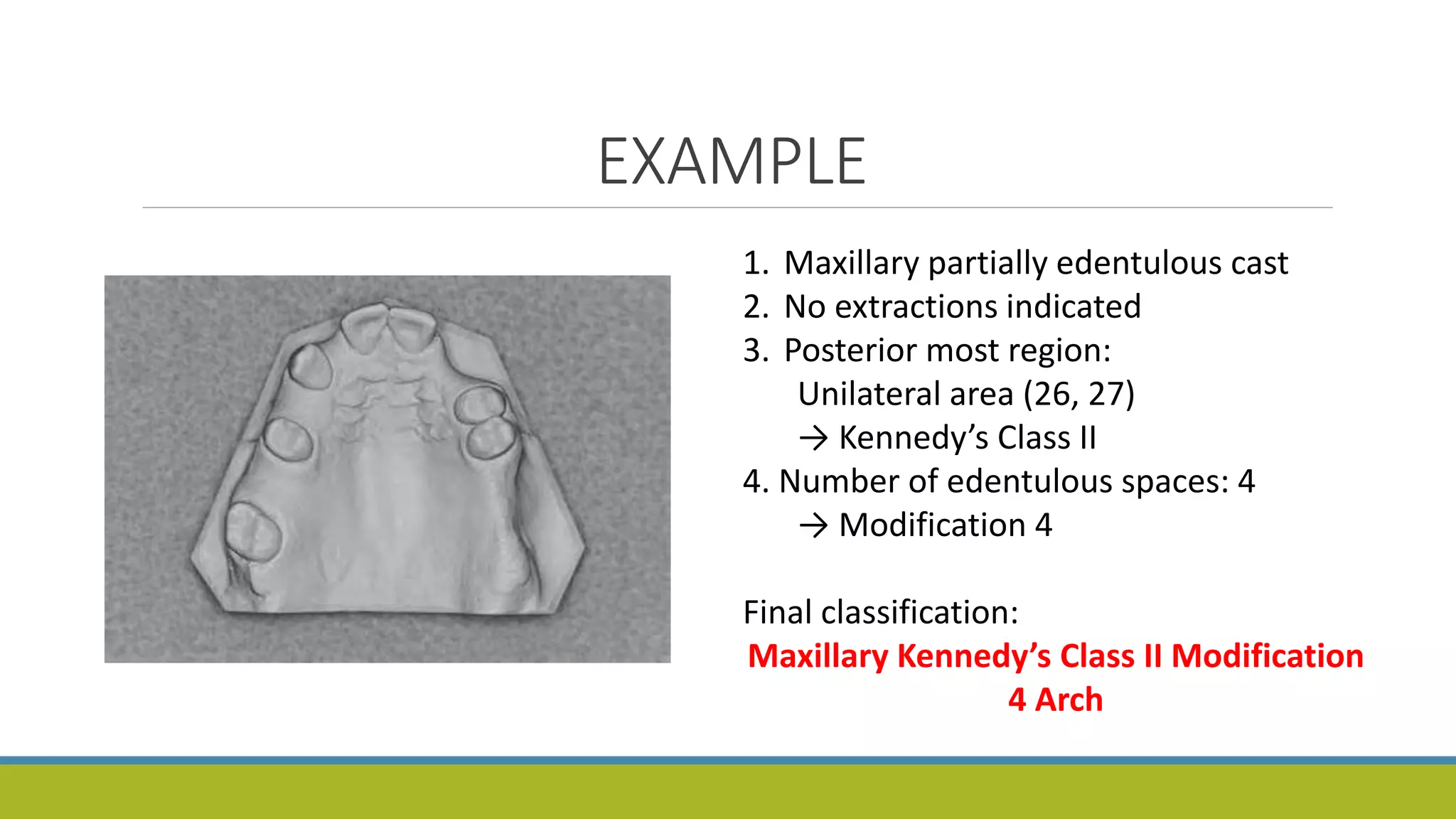
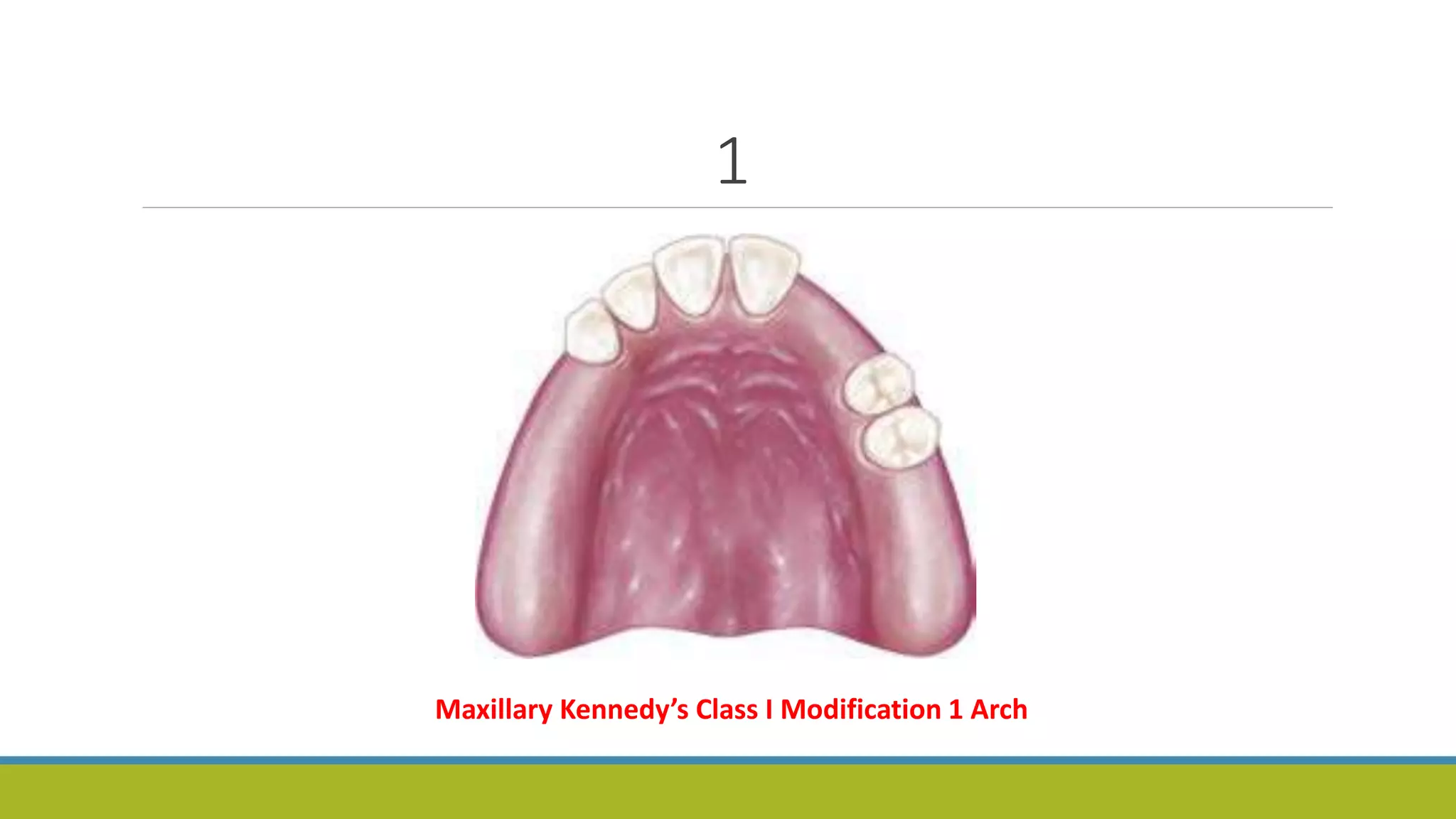
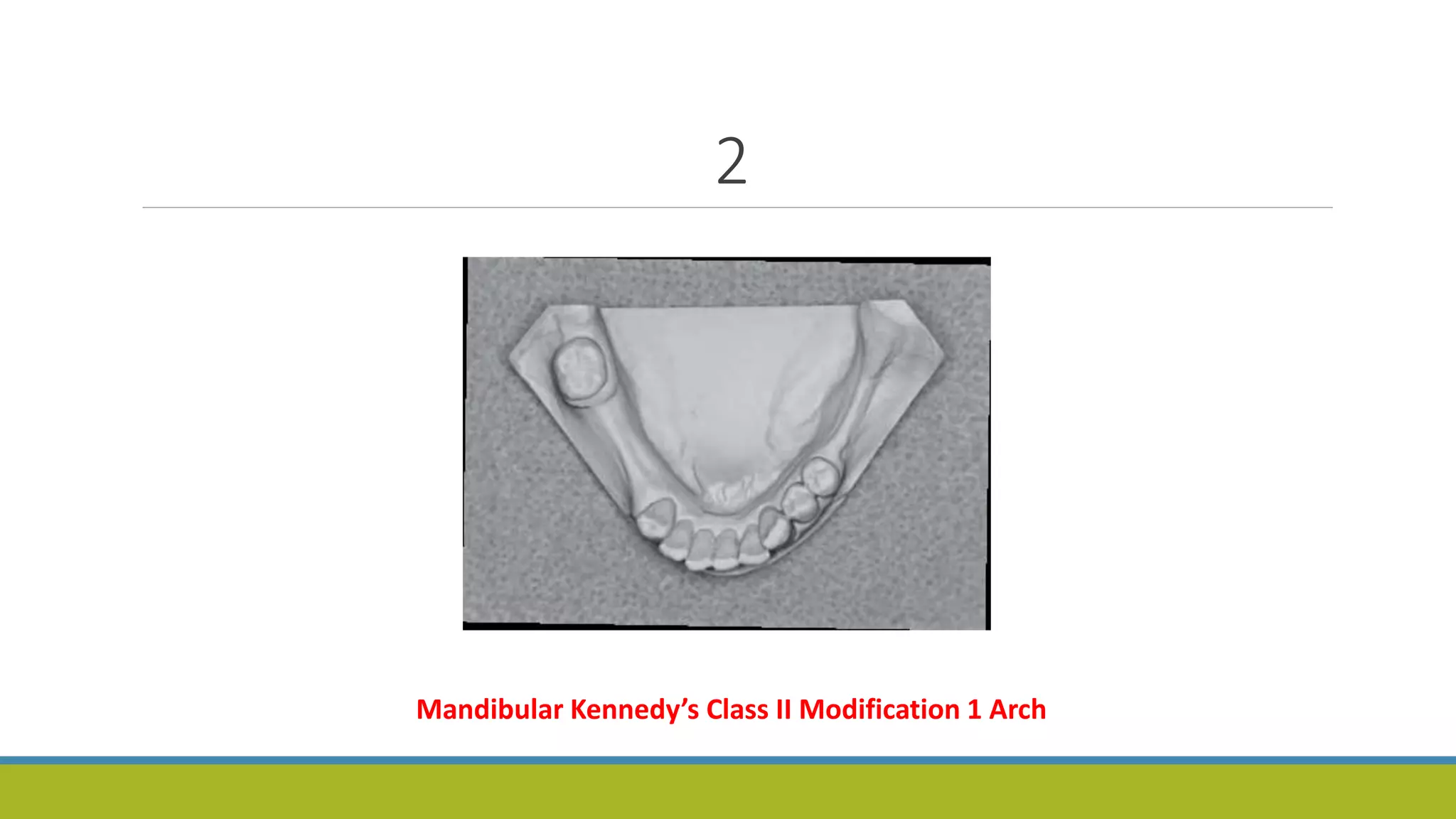
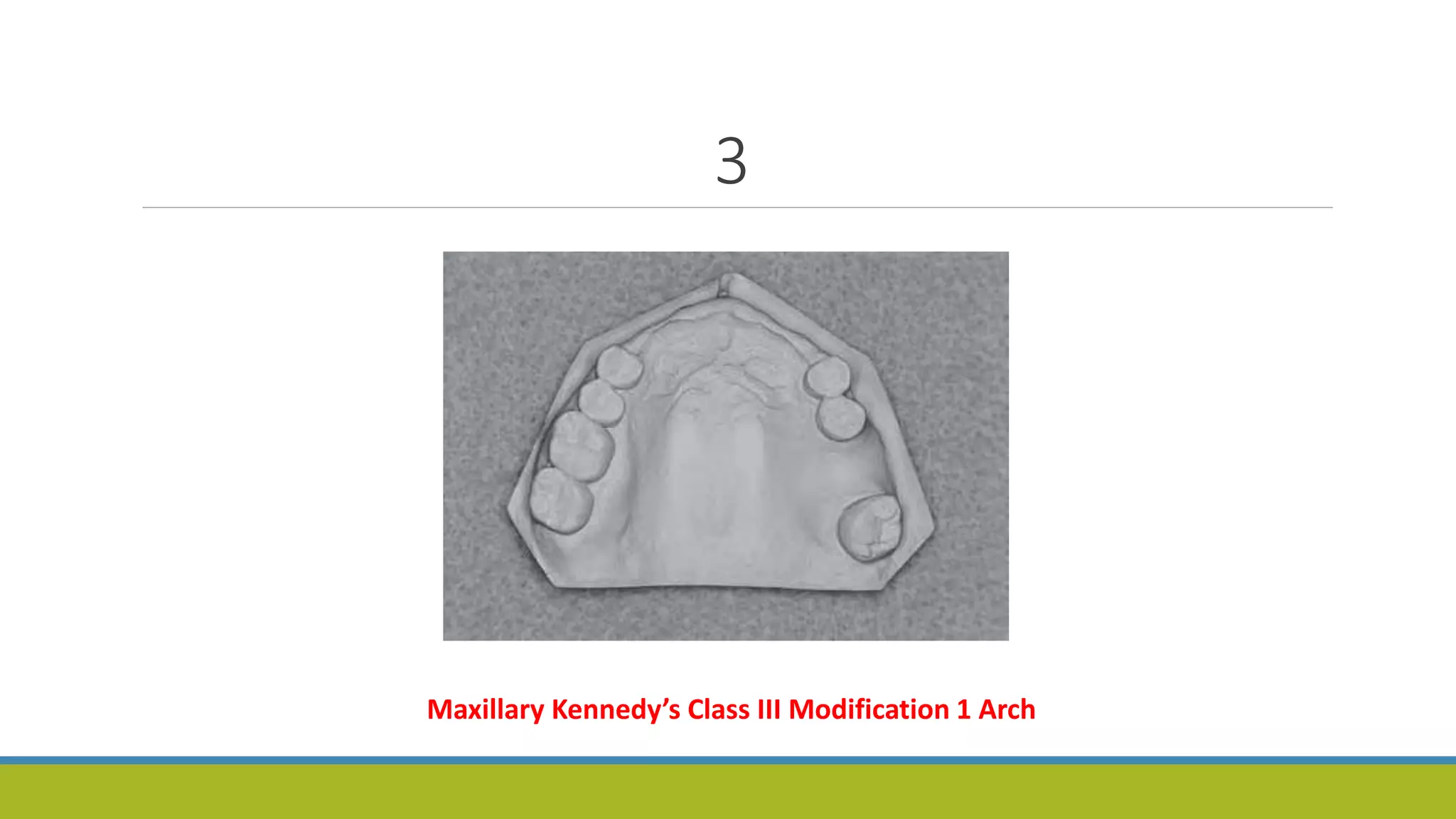
This document discusses Kennedy's classification system for partially edentulous arches and Applegate's rules for applying the Kennedy classification. It provides details on Kennedy's four basic classes for partial edentulism and Applegate's eight rules to govern the application of Kennedy's classification. Examples are given to demonstrate how to use Kennedy's classification and Applegate's rules to classify different clinical scenarios of partial edentulism.