
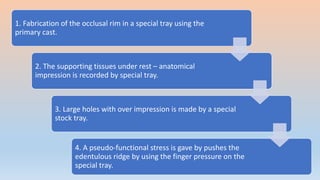

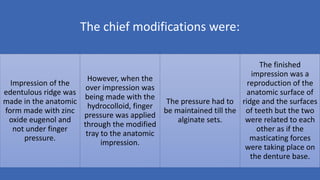

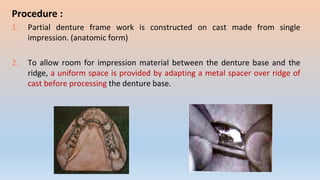
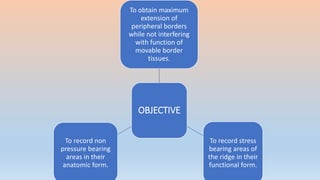
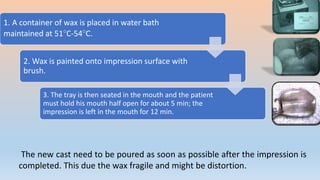
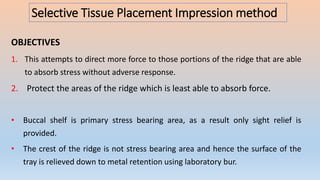
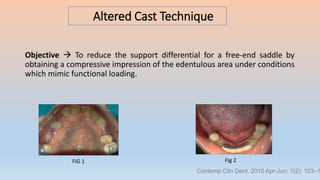

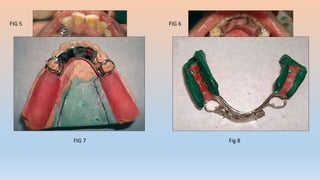
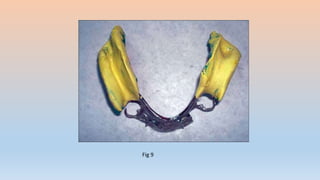
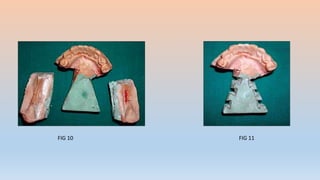




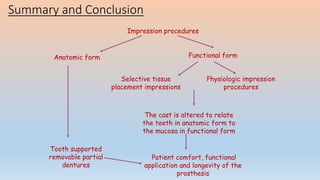


This document discusses impression procedures for removable partial dentures. It defines partial denture impressions and differentiates them from complete denture impressions. Various impression techniques are described including anatomic form impressions, functional impression techniques like McLean's method and the functional reline method. The document reviews literature on modified techniques like the altered cast technique and selective tissue placement impressions. It emphasizes the importance of functional impressions to distribute load and maximize longevity of remaining structures. In summary, the choice of impression technique impacts the support, function and longevity of the resulting removable partial denture.

















































































