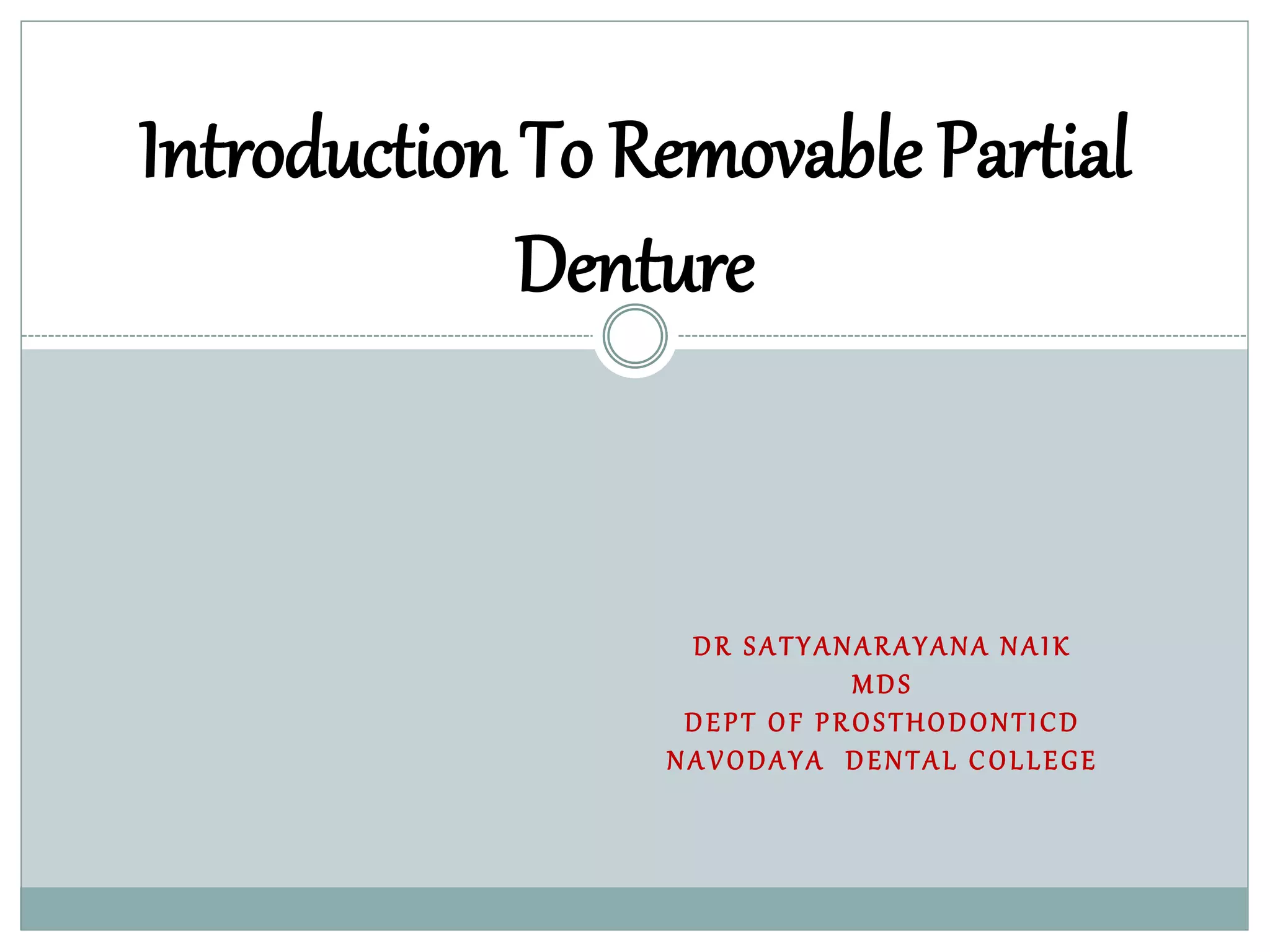
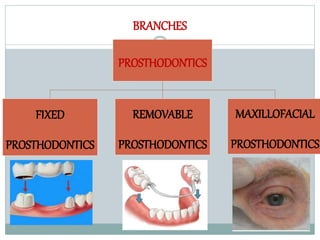
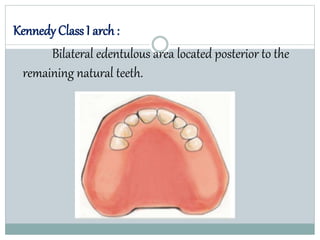
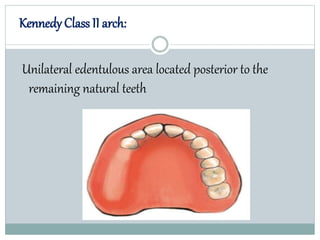
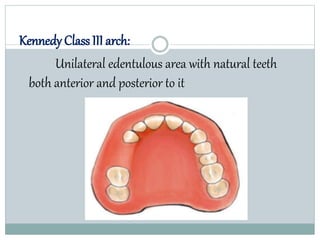
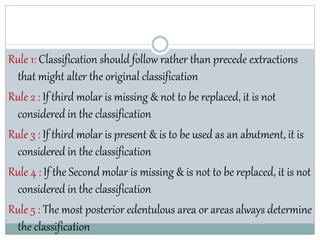
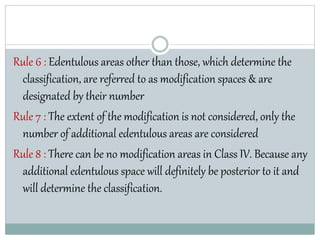
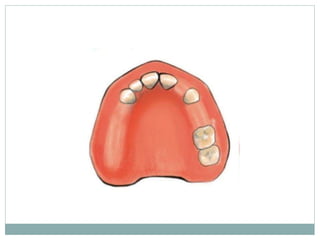
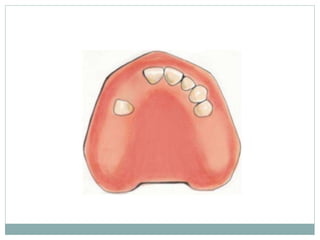
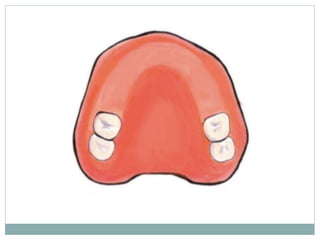
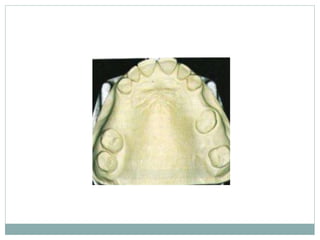
This document discusses removable partial dentures (RPDs) and classifications of partially edentulous arches. It begins by defining prosthodontics and RPDs. Kennedy's classification is then explained in detail, including the four major classes (I, II, III, IV). The classification assesses the location of edentulous spaces in relation to remaining teeth. Applegate later modified Kennedy's classification to include two additional classes (V, VI) based on abutment tooth condition. The document emphasizes that Kennedy's classification is widely accepted and aids in treatment planning for RPDs.