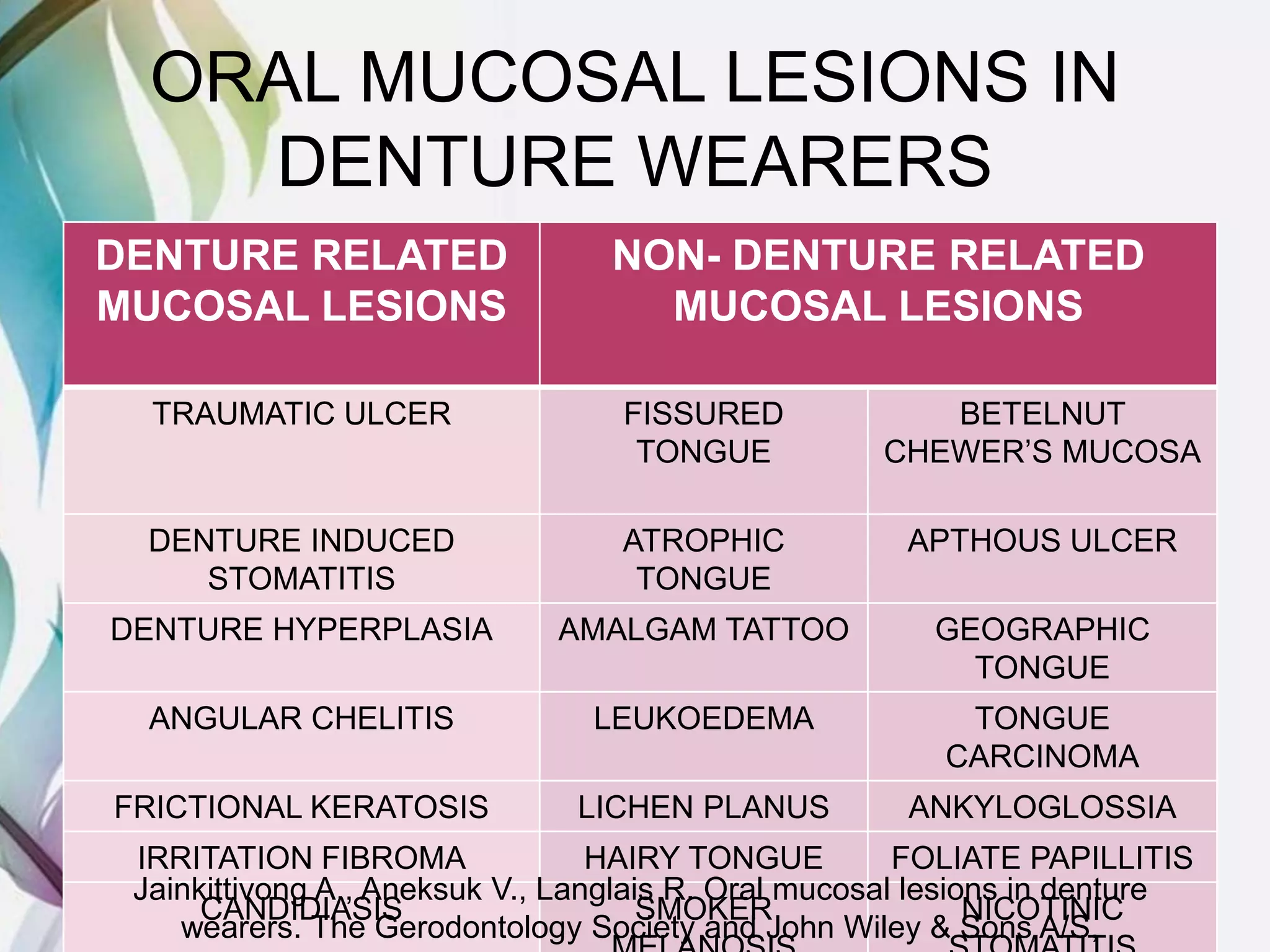
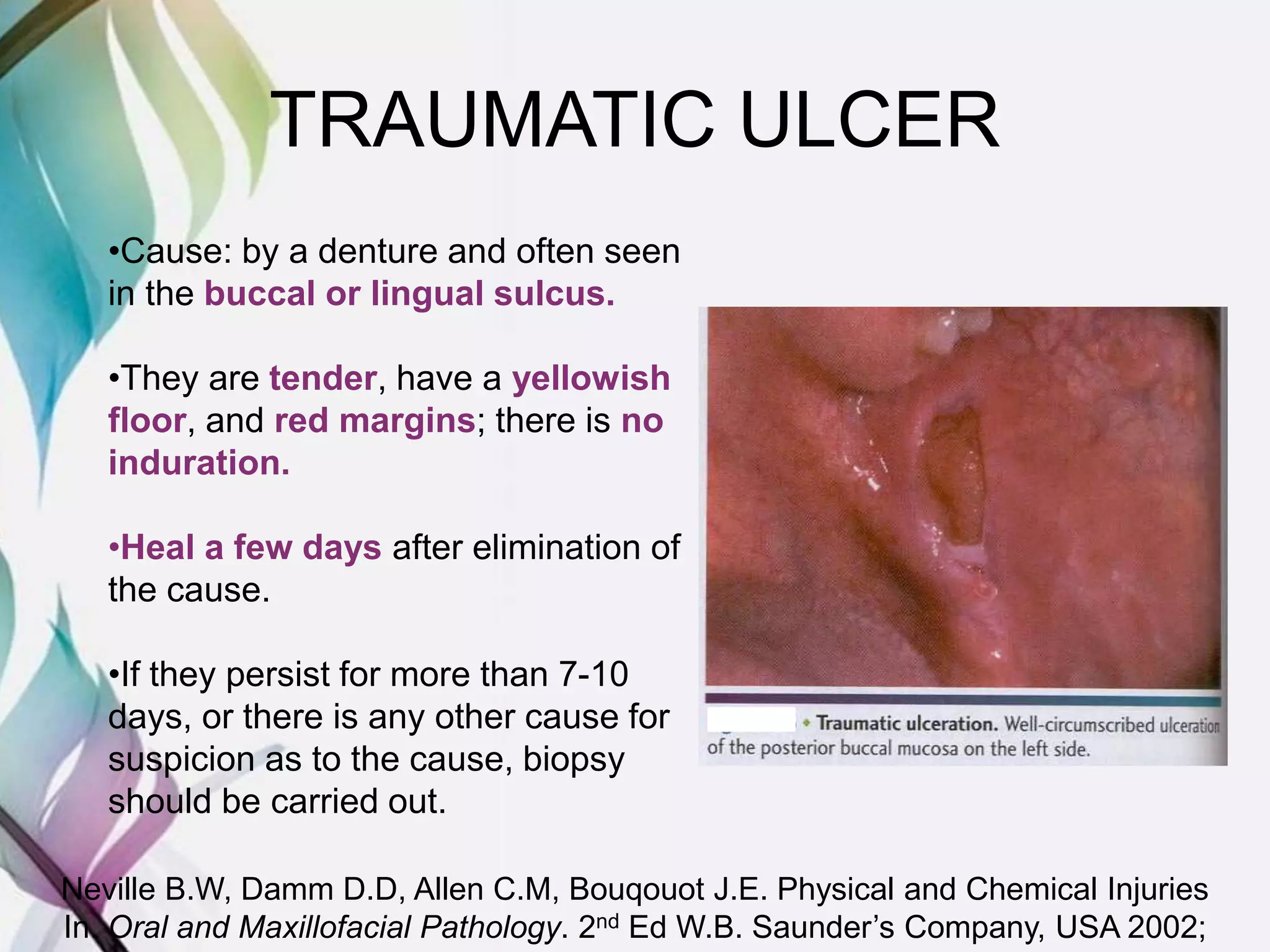
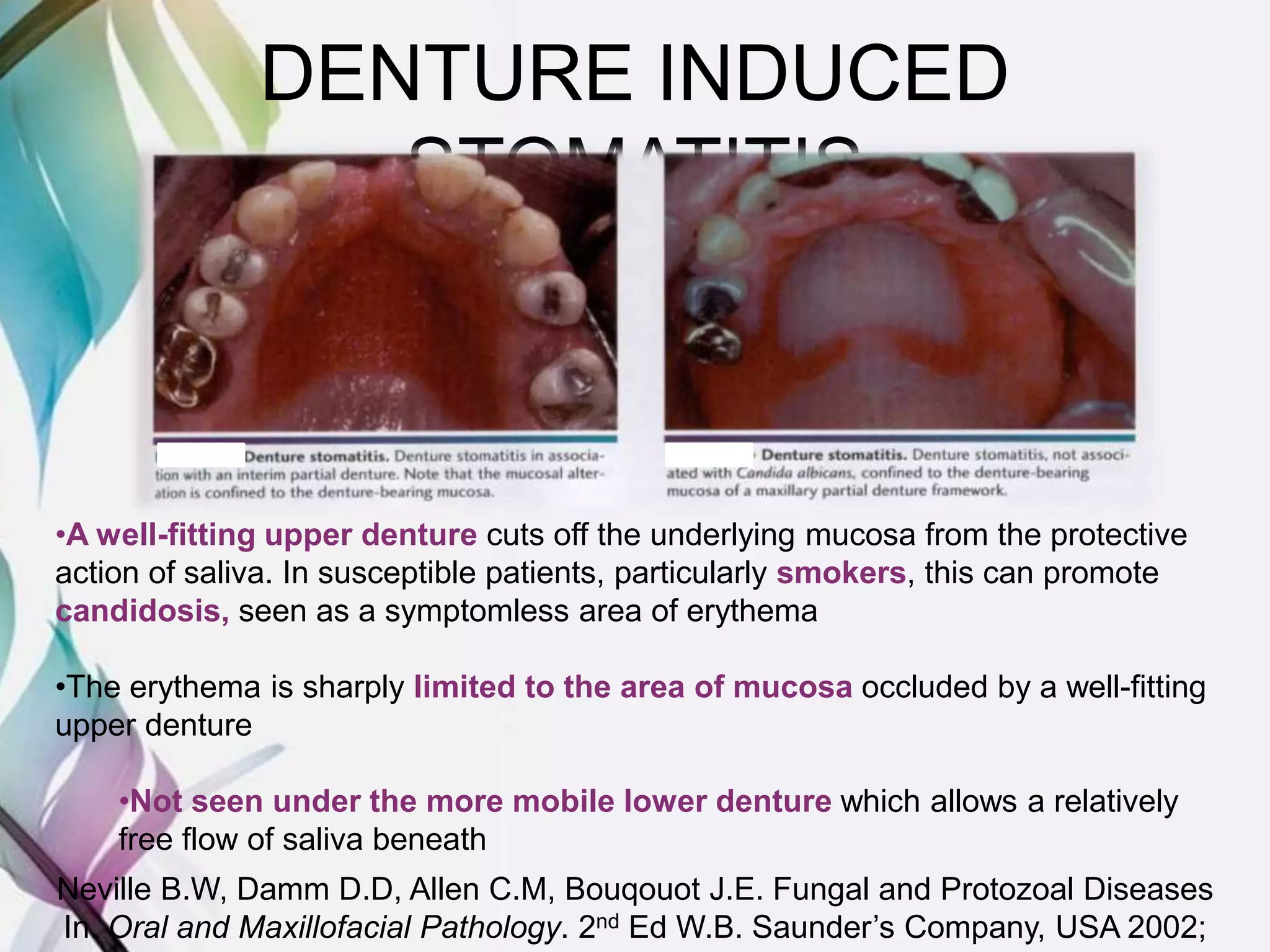
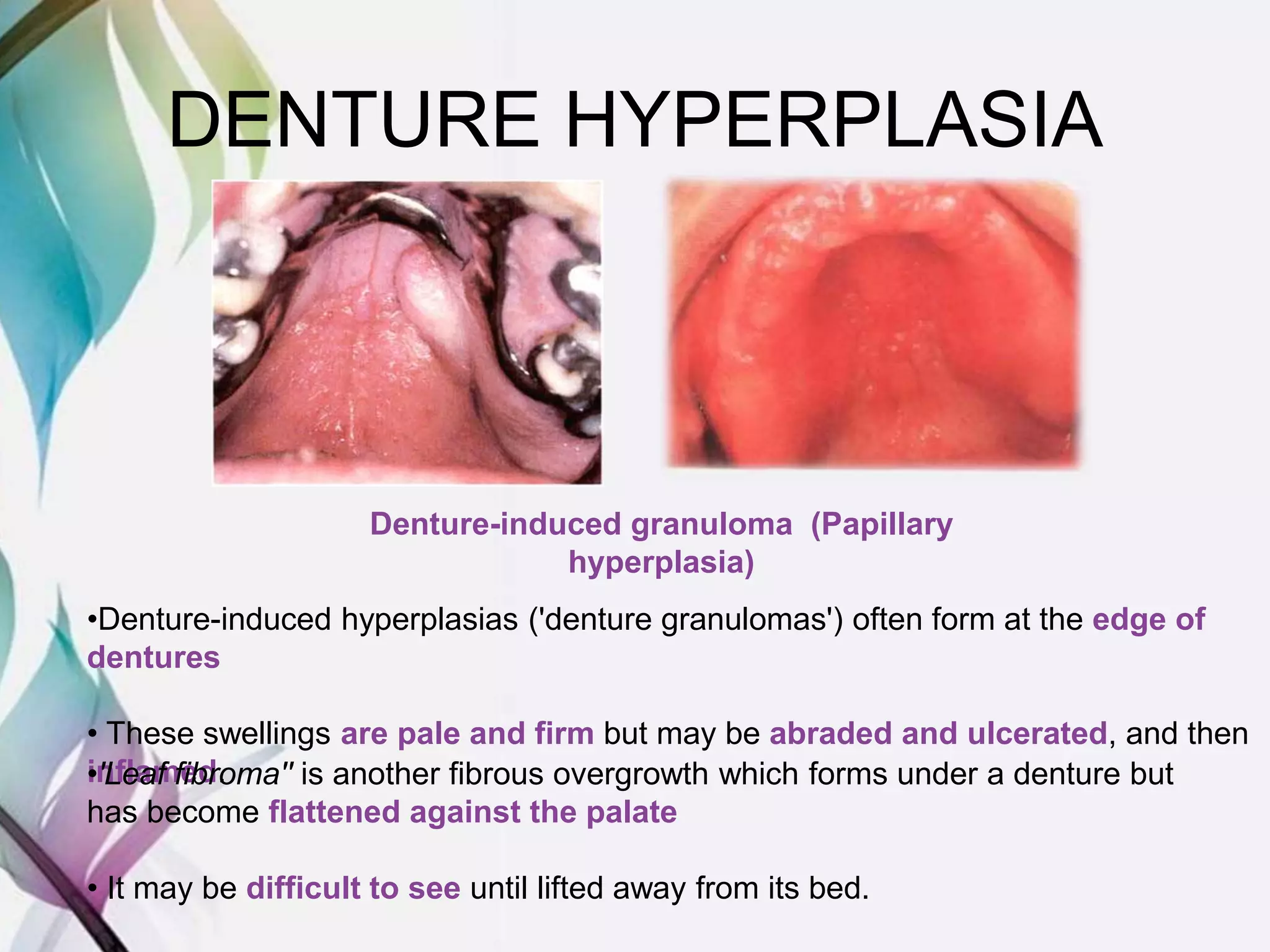
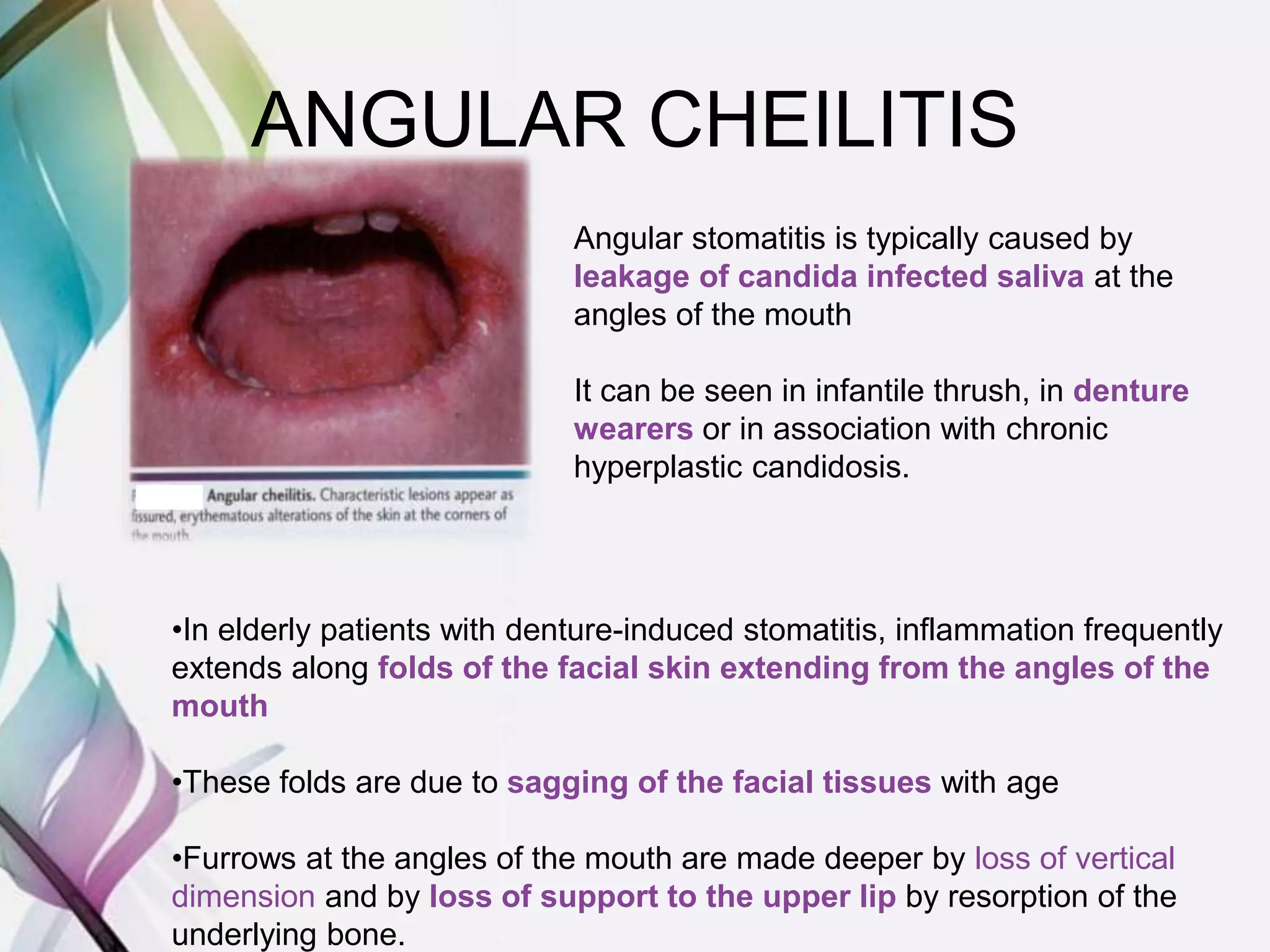
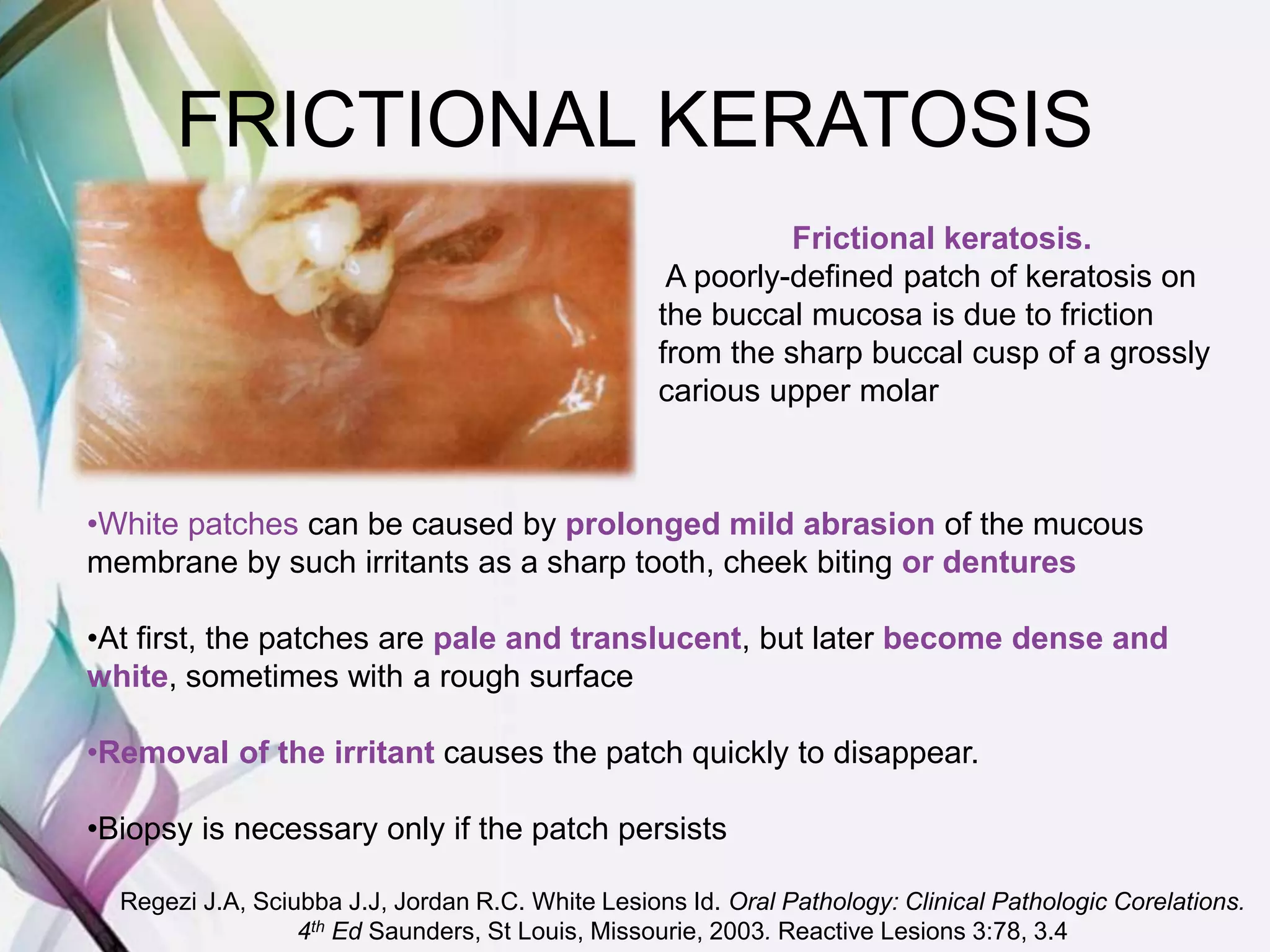
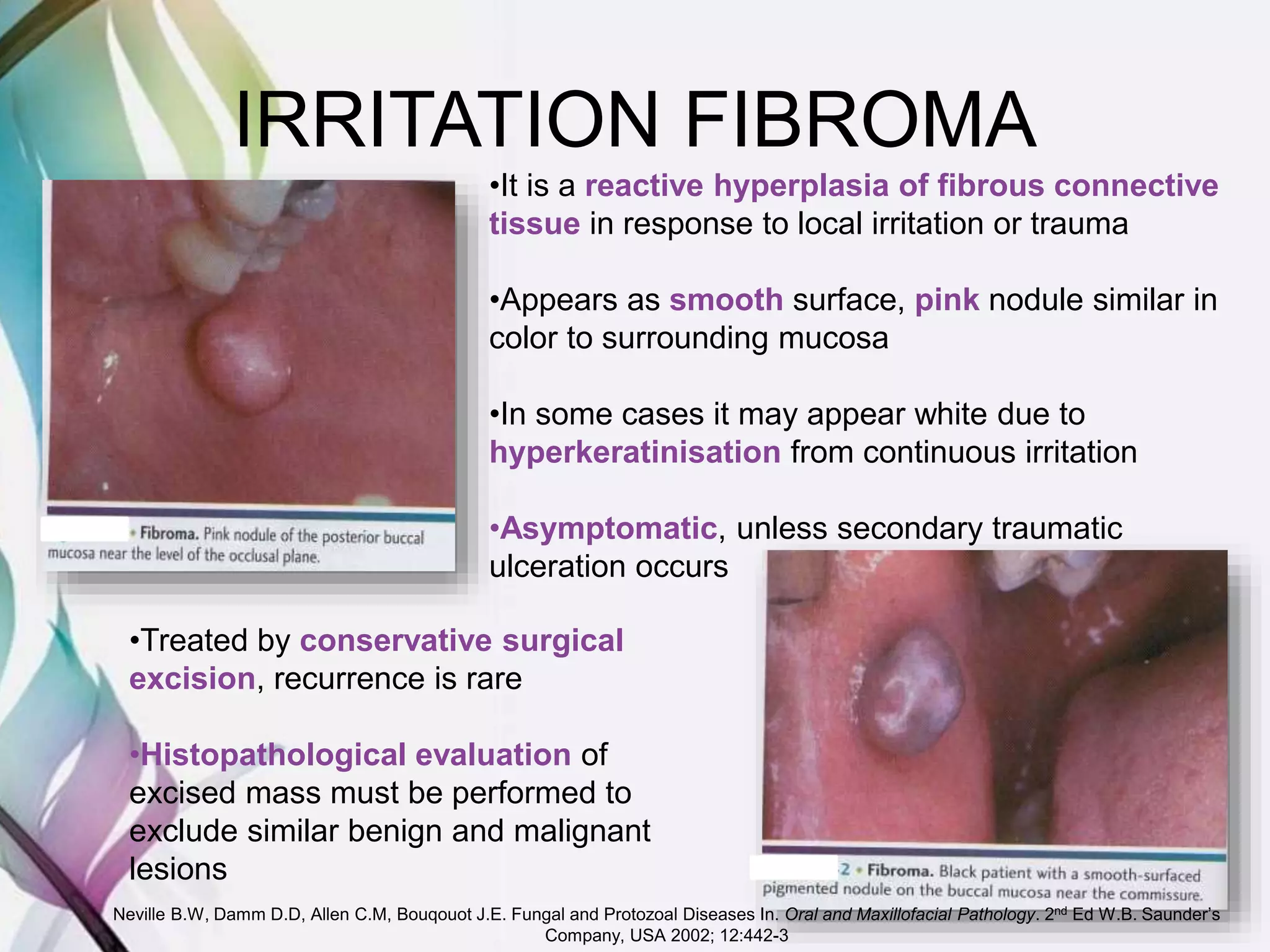
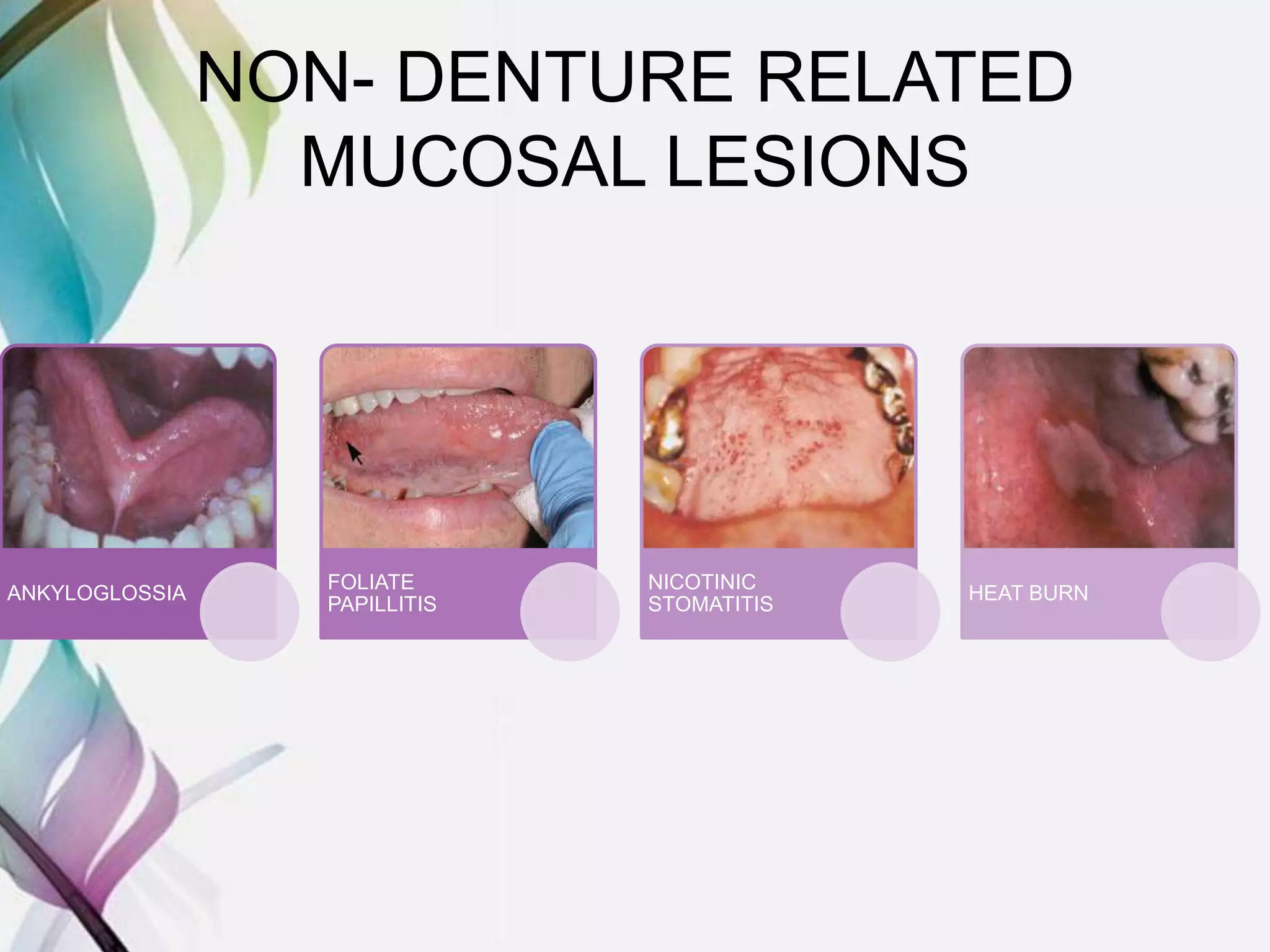
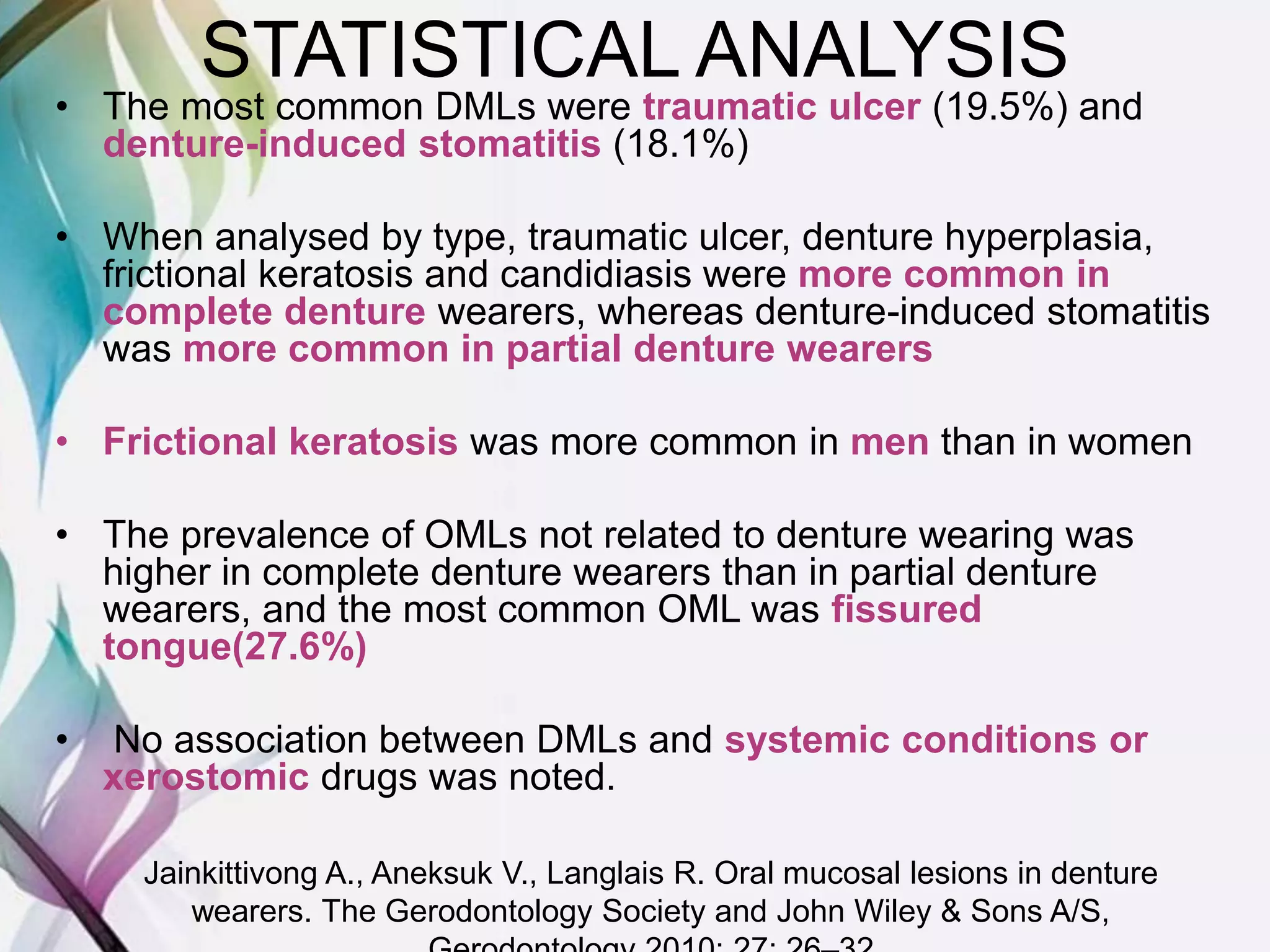
The document discusses oral mucosal lesions that can occur in denture wearers. It describes several types of denture-related mucosal lesions (DMLs) such as traumatic ulcers, denture-induced stomatitis, and denture hyperplasia. It also discusses non-denture related lesions including fissured tongue and lichen planus. A statistical analysis found the most common DMLs were traumatic ulcers and denture stomatitis. Complete denture wearers had higher rates of DMLs while partial denture wearers saw more stomatitis. The document provides details on clinical presentation and management of several specific oral lesions.