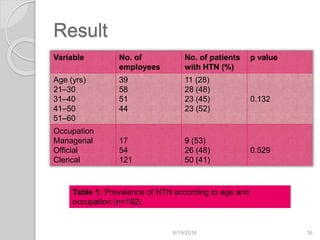
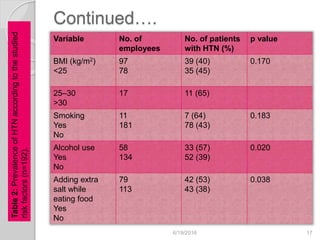
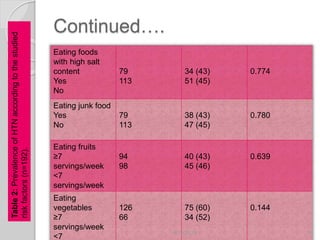
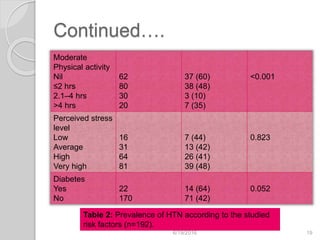
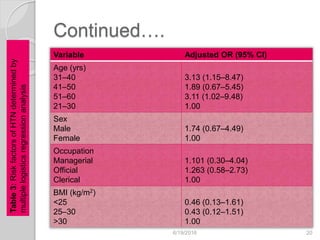
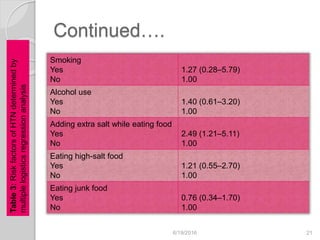
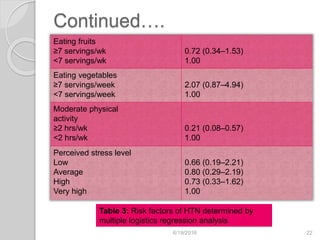
This study assessed the prevalence and risk factors of hypertension among 192 bank employees in Puducherry, India. The prevalence of hypertension was found to be 44.3%, with 55% being previously known cases and 45% newly diagnosed. Risk factors found to be significantly associated with hypertension included older age (over 40), alcohol use, adding extra salt while eating, and less physical activity of under 2 hours per week. The study provides valuable information on the risk factors for hypertension among this occupational group.




























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





