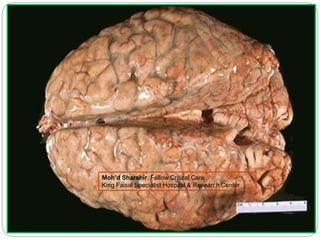
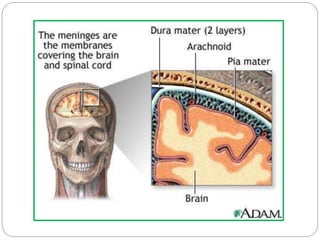
Meningitis is an inflammation of the meninges, the membranes surrounding the brain and spinal cord. It is caused by bacterial, viral, or fungal infections. The classic symptoms are fever, headache, and neck stiffness. Diagnosis involves examination of cerebrospinal fluid which shows increased white blood cells and decreased glucose levels in bacterial meningitis. Treatment depends on the identified pathogen but generally involves antibiotics. Adjunctive steroids may reduce complications for some types of bacterial meningitis. Outcomes vary depending on the cause, but bacterial meningitis can have mortality rates around 20% even with treatment.




![Role Of Steroids:
dexamethasone reduces cerebrospinal fluid (CSF)
concentrations of cytokines (such as tumor necrosis factor
[TNF]-alpha and interleukin [IL]-1), CSF inflammation, and
cerebral edema](https://image.slidesharecdn.com/casepresentationmeningitis-180610065229/85/Case-presentation-meningitis-and-treatment-Moh-d-Sharshir-41-320.jpg)
![ In patients with known or suspected
pneumococcal meningitis who are treated
with dexamethasone, we suggest
adding rifampin to the standard antibiotic regimen
(vancomycin plus
either ceftriaxone or cefotaxime) if susceptibility
studies show intermediate susceptibility
(minimum inhibitory concentration [MIC]
≥2 mcg/mL) to ceftriaxone and cefotaxime (Grade
2C). A reasonable alternative is to initiate rifampin
and then discontinue it if the isolate is susceptible
to the cephalosporin. (See 'Antibiotic
regimens' above.)](https://image.slidesharecdn.com/casepresentationmeningitis-180610065229/85/Case-presentation-meningitis-and-treatment-Moh-d-Sharshir-45-320.jpg)
![ In a prospective study of 86 adults with bacterial
meningitis, cerebral angiography was performed
in 27 (31 percent) because one or more of the
following findings were present: focal neurologic
deficits, abnormalities on computed tomographic
(CT) scanning, or persistent coma after three
days of antibiotic therapy [16]. Abnormal
angiograms were found in 13 of these 27
patients; the abnormal findings included:](https://image.slidesharecdn.com/casepresentationmeningitis-180610065229/85/Case-presentation-meningitis-and-treatment-Moh-d-Sharshir-49-320.jpg)
![ In another report, a cranial CT scan was
performed in 87 of 122 adults with bacterial
meningitis seen after 1975 [2]. A cerebral infarct
was noted in four, lesions consistent with septic
emboli in two and cavernous sinus thrombosis in
one. Four patients without a lesion on initial scan
had signs of an infarct on a later CT scan that
was performed because of persistent hemiparesis
in three and triplegia in one](https://image.slidesharecdn.com/casepresentationmeningitis-180610065229/85/Case-presentation-meningitis-and-treatment-Moh-d-Sharshir-51-320.jpg)


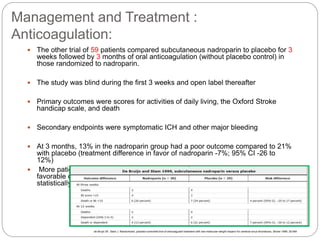
![Management and Treatment :
Anticoagulation:
In a nonrandomized case-control study, a greater proportion of
adult patients treated with LMWH (n = 119) compared with
unfractionated heparin (n = 302) were independent at six months
(92 versus 84 percent, adjusted odds ratio 2.4, 95% CI 1.0-5.7)
[33]. Treatment with LMWH was also associated with slightly
lower rates of mortality (6 versus 8 percent) and new intracranial
hemorrhage (10 versus 16 percent), but these outcomes were
not statistically significant
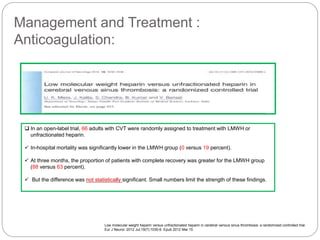
Unfractionated or low-molecular weight
heparin for the treatment of cerebral
venous thrombosis. Stroke.
2010;41(11):2575.](https://image.slidesharecdn.com/casepresentationmeningitis-180610065229/85/Case-presentation-meningitis-and-treatment-Moh-d-Sharshir-113-320.jpg)