Downloaded 47 times

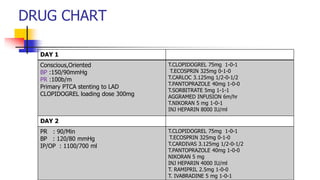
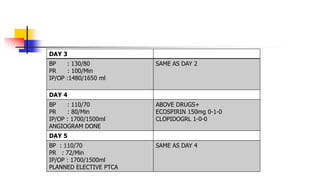
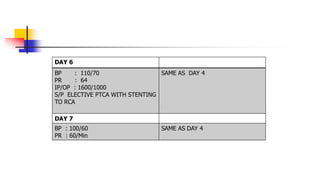
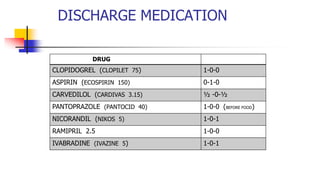
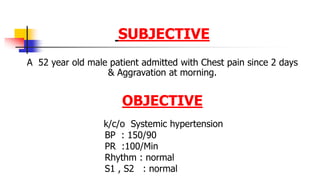
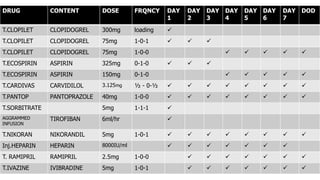
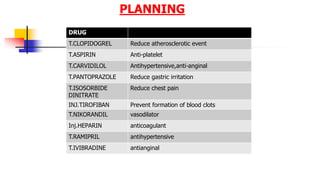


The document details the medical profile and treatment of a 52-year-old male patient diagnosed with anterolateral myocardial infarction and systemic hypertension following chest pain. After undergoing primary percutaneous coronary intervention (PTCA) with stenting, the patient's clinical progress and medication regimen over several days are outlined, including specific dosages and the rationale behind each drug administered. The document concludes with discussions on myocardial infarction causes, risk factors, and patient counseling points regarding medication and lifestyle changes.





















































































