Introduction
An estimated 1.13billion people worldwide have
HYPERTENSION, most of them (2/3rd) living in low &
middle-income countries.
Prevalence 30-40%, 24% in men & 20% women,
Prevalence > 60% in people aged >60 years
In 2015, 1 in 4 men & 1 in 5 women had HTN
Annual increase of 15-20% estimated by 2025
A major cause of premature death worldwide.
One of the global targets for Noncommunicable
diseases is to reduce the prevalence of
hypertension by 25% by 2025 (baseline 2010)
4.
Burden - India
NationalFamily Health Survey 2015-16
11% women and 15% in men were hypertensive
Prevalence was found to be higher in males and
those with high Body Mass Index.
Now – health & wellness center are focusing on
Noncommunicable Diseases and their prevention in
particular
5.
Symptoms of HTN
Hypertensionis called a "silent killer“
Most people with HTN are unaware of their status
as they have no warning signs or symptoms
It is essential to get blood pressure measured
regularly.
When symptoms do occur, they are early morning
headaches, nosebleeds, irregular heart rhythms,
vision changes & buzzing in the ears
6.
Symptoms of HTN
Severehypertension can cause fatigue, nausea,
vomiting, confusion, anxiety, chest pain & muscle
tremors.
The only way to detect hypertension is to
measure
7.
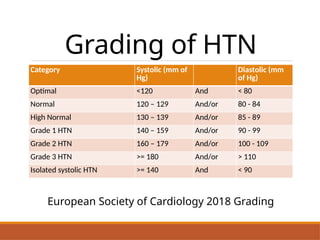
Grading of HTN
CategorySystolic (mm of
Hg)
Diastolic (mm
of Hg)
Optimal <120 And < 80
Normal 120 – 129 And/or 80 - 84
High Normal 130 – 139 And/or 85 - 89
Grade 1 HTN 140 – 159 And/or 90 - 99
Grade 2 HTN 160 – 179 And/or 100 - 109
Grade 3 HTN >= 180 And/or > 110
Isolated systolic HTN >= 140 And < 90
European Society of Cardiology 2018 Grading
8.
Classification
Primary [Essential]
Cause unknown,accounts for 90% cases, most
common
Secondary
Some other disease process or abnormality
involved in causation, like kidney disease, adrenal
gland disorder, narrowing of Aorta, toxemia of
pregnancy, altogether less than 10% cases
9.
Risk Factors ofHTN
NON MODIFIABLE
1) Age – BP increases with age in both sexes due
to accumulation of environmental factors and
ageing phenomenon
2) Sex – in adolescence Men display higher
average, difference is clearly evident in young &
adults. Later on this pattern narrows & may
even reverse. Post menopausal changes are
contributory.
.
10.
Risk Factors ofHTN
3) Genetic factors – evidence suggests BP levels
are determined partly by genetic factors, with
polygenic inheritance.
Twin studies - BP of monozygotic twins are strongly
related than zygotic twins. In contrast no relation
was found in levels of husband & wife, and between
adopted children.
Family studies – children of 2 normotensive parents
have 3% possibility of developing HTN, while it is
45% for hypertensive parents
.
11.
Risk Factors ofHTN
4) Ethnicity – Population studies have shown
higher levels in black population
MODIFIABLE
1. OBESITY – Greater the wt. gain greater the risk.
On loosing weight the BP also decreases.
“Central obesity” has been positively correlated
with high BP
2. SALT INTAKE – high intake 7-8 g/day increases
the risk. Low sodium intake decreases the BP.
Japan sodium intake is above 400 mmol/day has
higher incidence
.
12.
Risk Factors ofHTN
3) SATURATED FAT – It raises BP & serum
cholesterol. Cholesterol & LDL are involved in
atherosclerosis.
Recommended – greater intake of PUFA and less
intake of saturated fat. Fat intake should be less
than 30% of total calories.
4) DIETARY FIBRE – beneficial in reducing total &
LDL cholesterol.
5) ALCOHOL INTAKE
.
13.
Risk Factors ofHTN
6) HEART RATE – hypertensive subjects were found
to have higher heart rate. This may be due to
resetting of sympathetic activity at a higher level
7) PHYSICAL INACTIVITY – minimum of 30 minutes
for at least 5 days a week is essential to reduce
the risk of HTN and NCD. Sedentary lifestyle
leads to obesity and predisposes to NCD
.
14.
Risk Factors ofHTN
6) ENVIRONMENTAL STRESS – higher
noradrenaline in hypertensive supports that
over activity of sympathetic system is involved.
9) SOCIO-ECONOMIC STATUS – earlier higher
disease burden in developed countries, but now
the trend is transitioning. More cases in low &
middle income countries.
.
15.
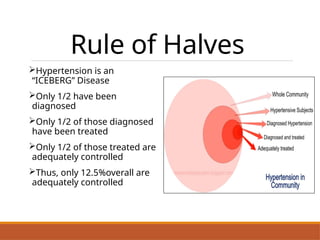
Rule of Halves
Hypertensionis an
“ICEBERG” Disease
Only 1/2 have been
diagnosed
Only 1/2 of those diagnosed
have been treated
Only 1/2 of those treated are
adequately controlled
Thus, only 12.5%overall are
adequately controlled
16.
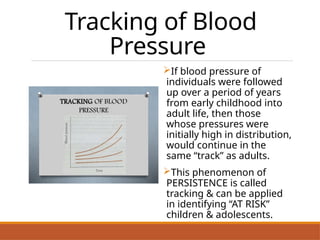
Tracking of Blood
Pressure
Ifblood pressure of
individuals were followed
up over a period of years
from early childhood into
adult life, then those
whose pressures were
initially high in distribution,
would continue in the
same “track” as adults.
This phenomenon of
PERSISTENCE is called
tracking & can be applied
in identifying “AT RISK”
children & adolescents.
17.
Prevention
WHO recommended approach:
1.Primary Prevention- “all measures to reduce the
incidence of disease in population by reducing
RISK of onset”
a. Population Strategy
b. High Risk Strategy
2. Secondary Prevention
We can control hypertension by medication
(secondary) but the ultimate goal is PRIMARY
Prevention
18.
Population Strategy-
for All
Evena small reduction in
average BP of Population
would produce large
reduction in incidence of
CVD complications.
GOAL – to shift the BP
towards lower levels with
multifactorial approach &
non Pharmacotherapeutic
interventions
Interventions
Nutrition – DASH
(dietary approach to
stop HTN), low sodium
& fat
Weight reduction –
maintain BMI < 25
Exercise promotion
Behavioural changes
Health Education
Self Care
19.
High - RiskStrategy
GOAL – To prevent the attainment of levels of
blood pressure which requires treatment.
Appropriate for community with low prevalence of
risk factors
Detection of High RISK subjects by assessing all
predisposing factors & clinical methods
Interventions to identify those at Higher RISK
Tracking of Blood Pressure from childhood
Family History details of hypertension
20.
Secondary
Prevention
GOAL – Todetect & control high BP of effected
individual
1) Early Case detection – major problem,
remember silent killer and iceberg
phenomenon. SCREENING of population with
adequate follow up
2) Treatment - modern Anti-hypertensive therapy
3) Patient compliance – “the extent to which the
patients behaviour coincides with clinical
prescription” . Health education improves
compliance
it’s a control and not cure so has to be LIFELONG
21.
Treatment
India Hypertension ManagementInitiative
(in collaboration with ICMR)
Measure BP of all above 30 years
If SBP >= 140 and/or DBP >= 90 mm of Hg
then follow.
Newer initiatives for
NCD
Screeningat all levels in the health care delivery
system from sub-centre & above
Capacity building at various levels of health care
for prevention, early diagnosis, treatment,
rehabilitation, IEC/BCC, operational research and
rehabilitation.
To support for development of database of NCDs
through Surveillance System and to monitor NCD
morbidity and mortality and risk factors.
Health promotion through behaviour change with
involvement of community, civil society, community
based organizations, media etc.

![Classification
Primary [Essential]
Cause unknown, accounts for 90% cases, most
common
Secondary
Some other disease process or abnormality
involved in causation, like kidney disease, adrenal
gland disorder, narrowing of Aorta, toxemia of
pregnancy, altogether less than 10% cases](https://image.slidesharecdn.com/htn-250627160749-c9527b5d/85/HTN-epid-previous-control-and-management-l-pptx-8-320.jpg)