Download as PDF, PPTX
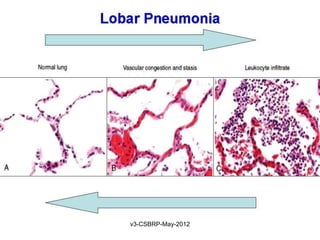

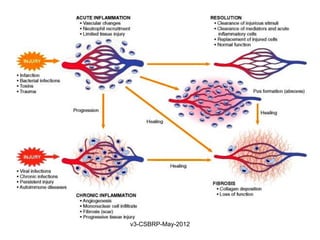

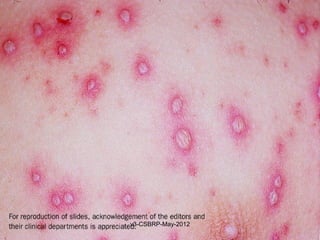
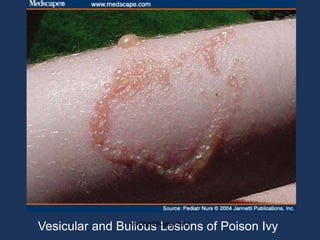


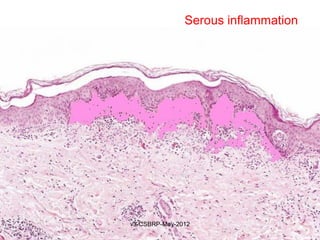
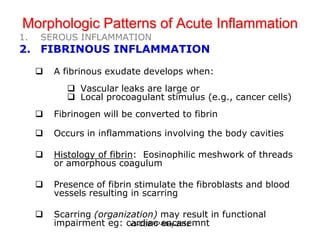
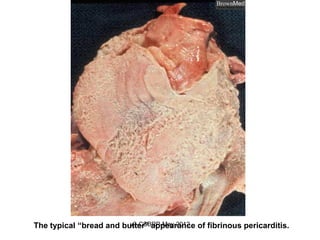

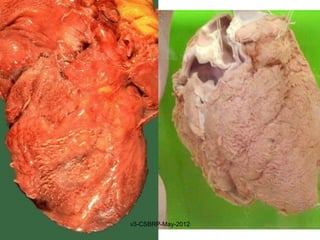
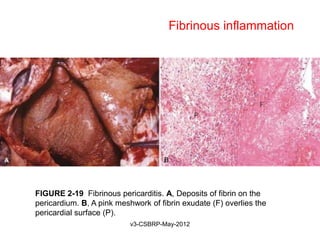
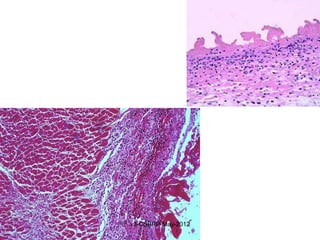


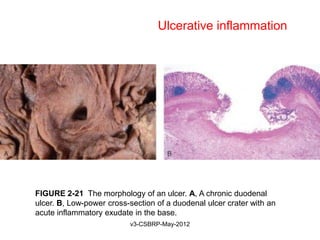
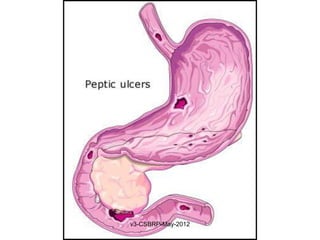



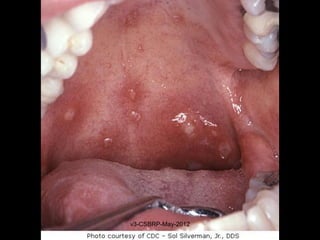


The document discusses the outcomes of acute inflammation and their morphological patterns. There are three potential outcomes of acute inflammation: 1) complete resolution, 2) healing by fibrosis, or 3) chronic inflammation. It also describes four main morphological patterns of acute inflammation: serous, fibrinous, suppurative (abscess formation), and ulcerative. Each pattern is associated with different clinical presentations and histological features.

































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









