Downloaded 491 times












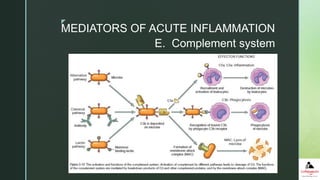
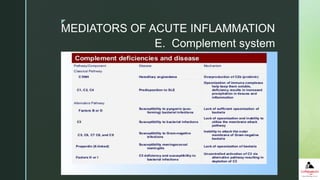

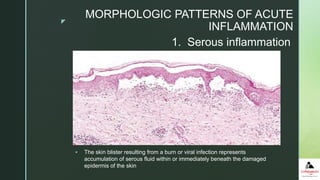













The document provides a comprehensive overview of inflammation and repair, detailing the definitions, types (acute and chronic), causes, and steps involved in inflammation. It explains the harmful consequences of misdirected inflammation, various mediators, and morphological patterns associated with both acute and chronic inflammation. Additionally, it discusses tissue repair mechanisms and the factors influencing them, highlighting specific examples of healing processes.























































































