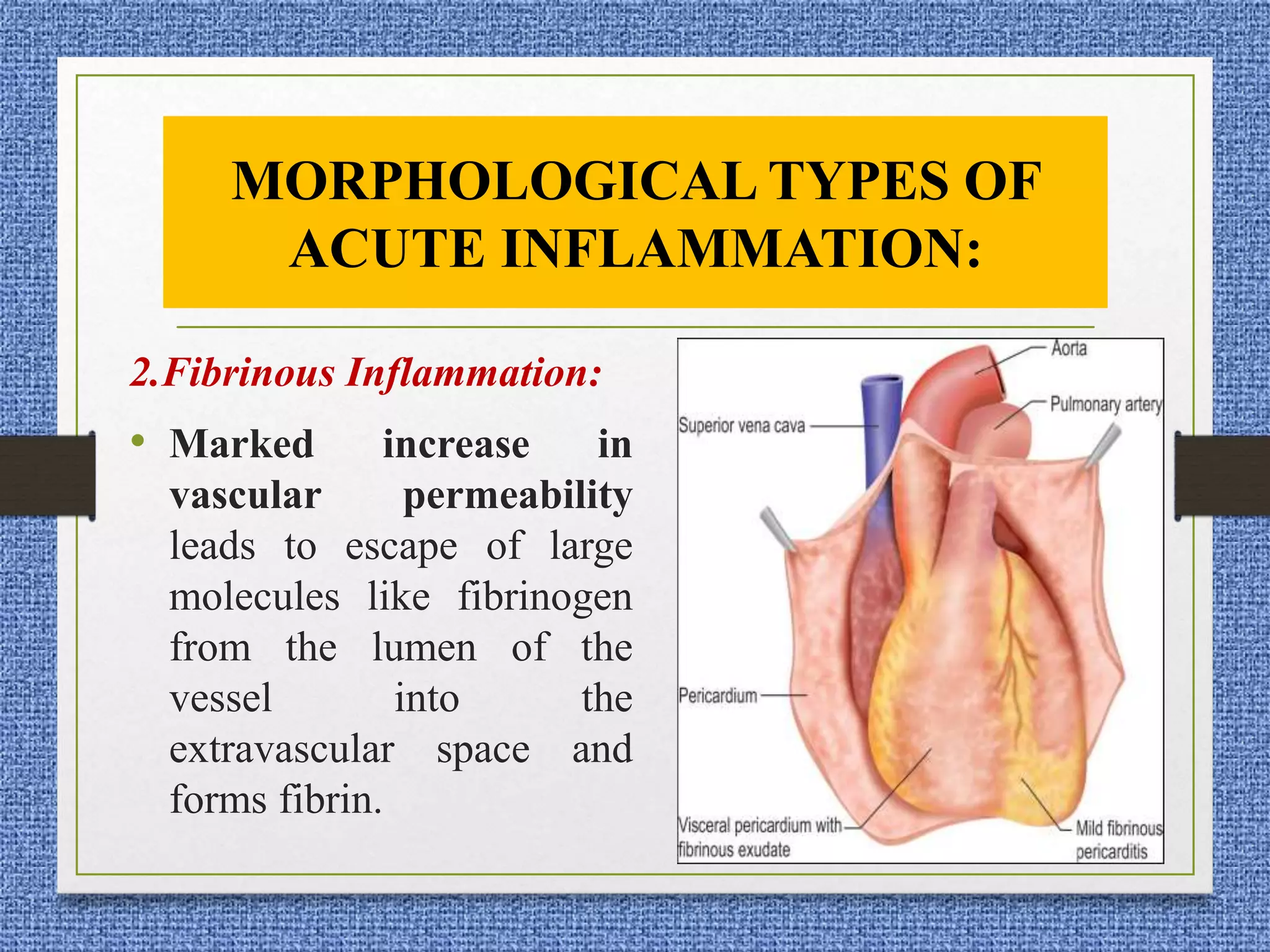
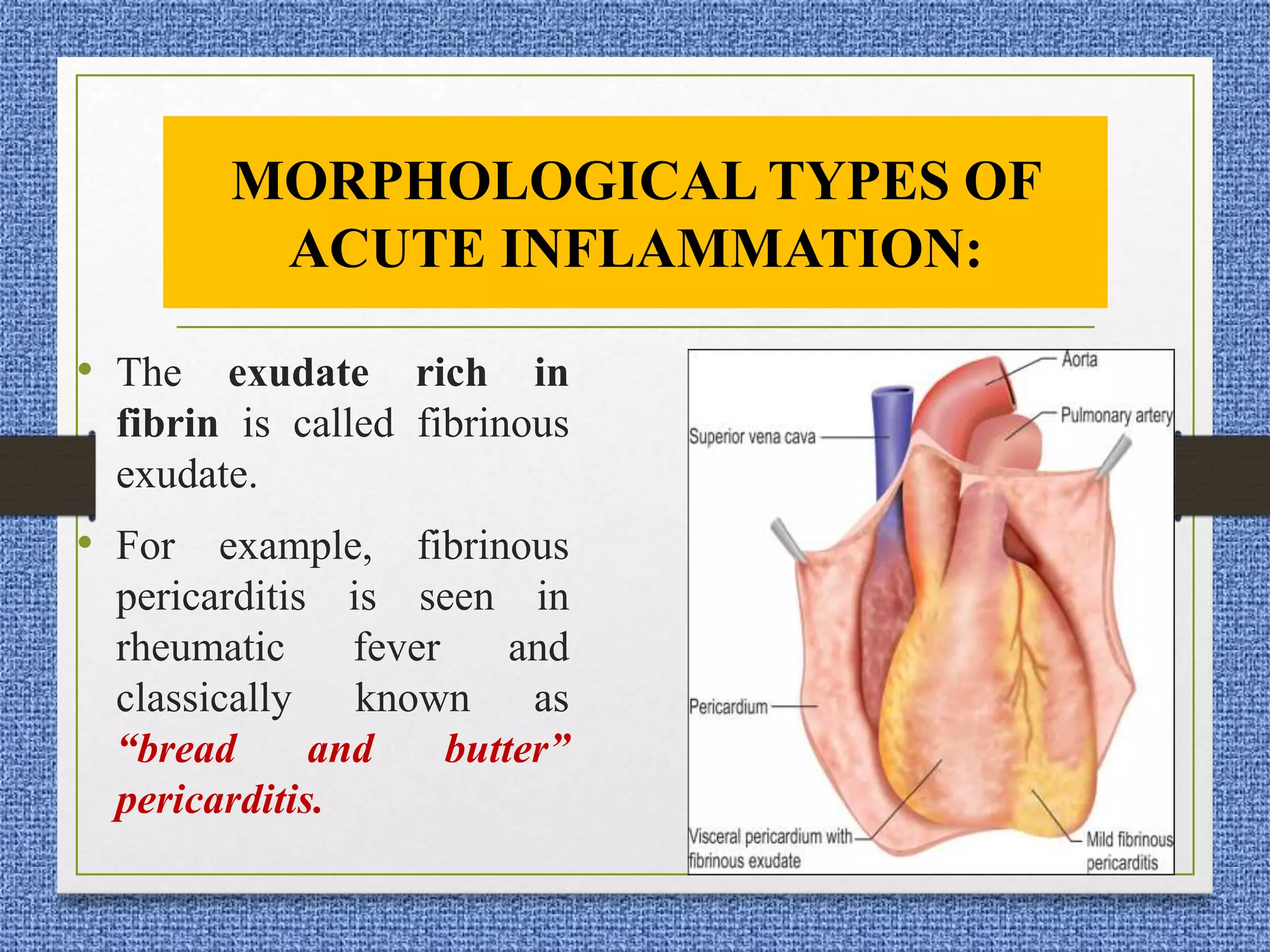
1. The document describes the different morphological patterns of acute inflammation including serous, fibrinous, suppurative, hemorrhagic, catarrhal, membranous, and necrotizing inflammation.
2. It also discusses the systemic effects of acute inflammation known as the acute phase response, including fever, increased acute phase proteins, and changes in white blood cells.
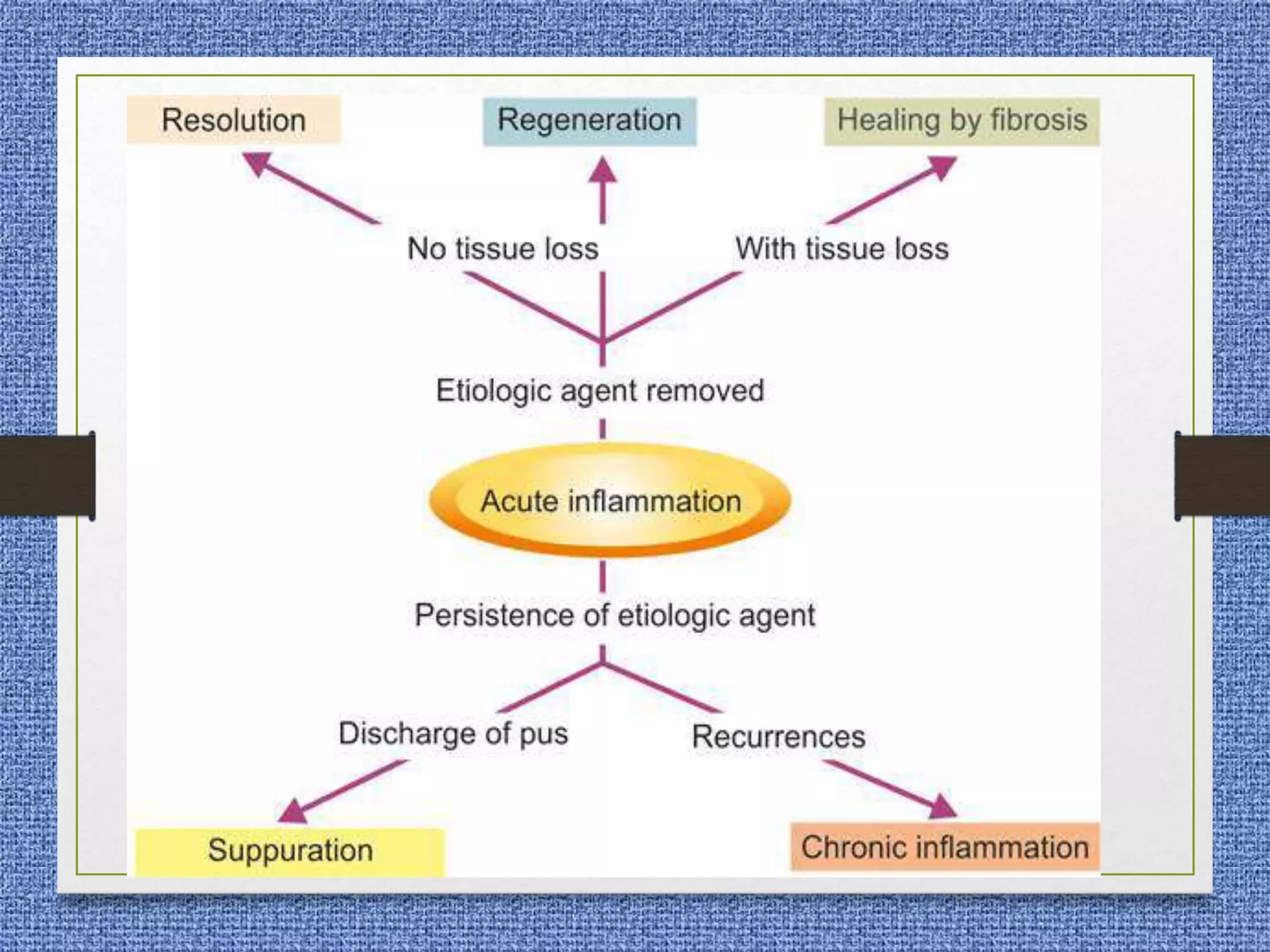
3. The fates of acute inflammation are described as resolution, healing, suppuration, or progression to chronic inflammation.