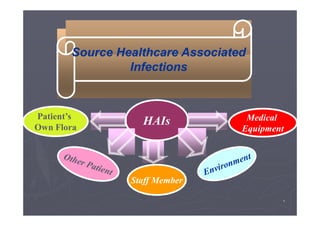
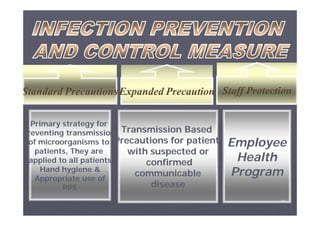
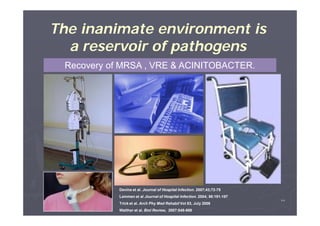
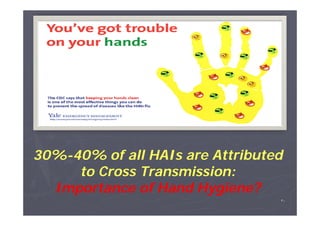
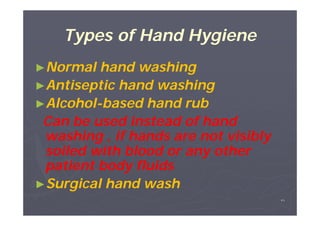
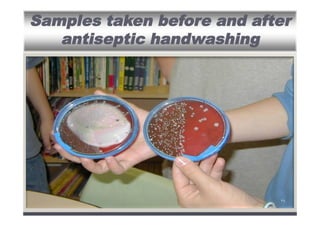
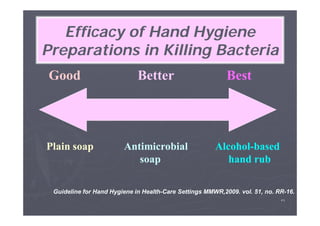
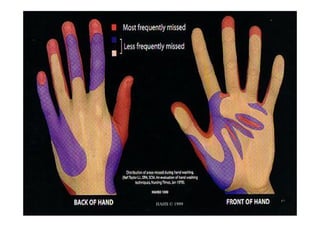
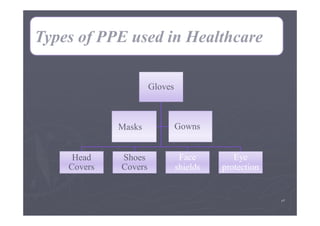
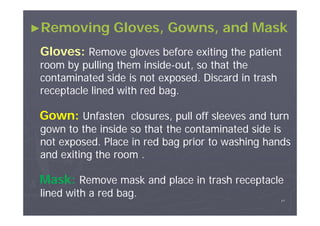
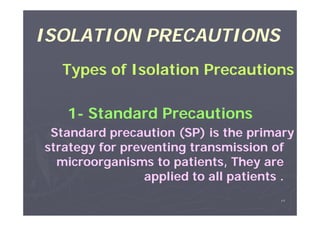
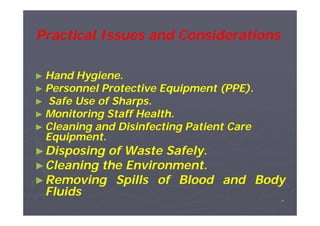
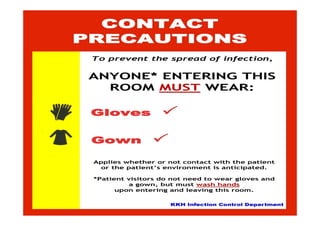
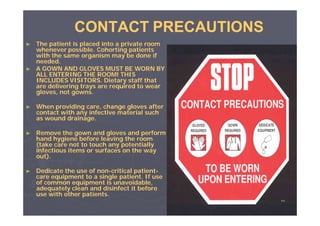
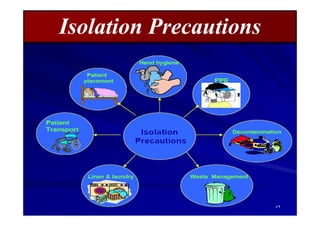
The document outlines the importance of infection control in healthcare settings to ensure patient, staff, and visitor safety. It emphasizes the rise in healthcare-associated infections (HAIs) and the necessity of coordinated infection control programs that include hand hygiene, use of personal protective equipment (PPE), and effective organizational policies. The goal is to reduce infection risks through comprehensive strategies that involve all healthcare personnel in preventive measures.















































































![Infection Control Guidelines for Physiotherapy Services[compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforphysiotherapycompatibilitymode-131231001808-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





























![Employee's' health clinic orientation [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/employeeshealthclinicorientationcompatibilitymode-140123022438-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Barrier technique personal protective equipment [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/barriertechnique-personalprotectiveequipmentcompatibilitymode-140123022003-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Barrier technique hand hygiene [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/barriertechnique-handhygienecompatibilitymode-140123021839-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![التعريف العام نعيادة صحة العاملين [Compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/compatibilitymode-140123021257-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Sharp Injuries Prevention[compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/sharpinjuriespreventioncompatibilitymode-131231014416-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
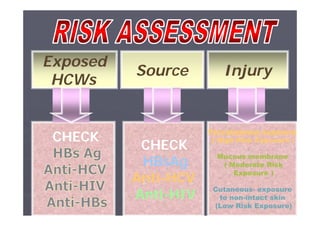
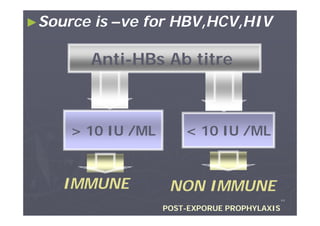
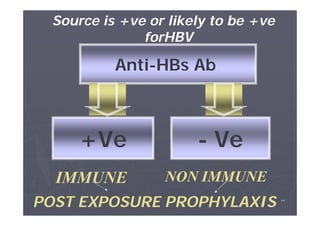
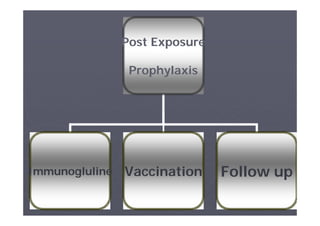
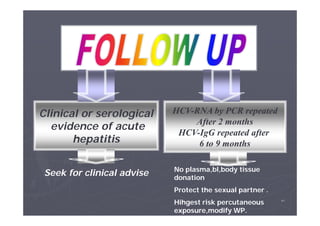
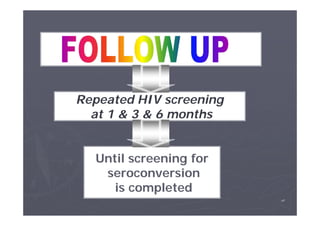
![Sharp injuries and needle stick post exposure prophylaxis [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/sharpinjuriesandneedlestickpostexposureprophylaxiscompatibilitymode-131231013025-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Role of infection control in patient safety [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/roleofinfectioncontrolinpatientsafetycompatibilitymode-131231012445-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Prevention of Surgical Site Infection- SSI [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/preventionofssicompatibilitymode-131231011316-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

![Infection Control Guidelines in Tuberculosis [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/infectioncontrolguidlinesintuberculosiscompatibilitymode-131231005155-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



![Infection Control Guidelines for Ophthalmology Clinic [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforophthalmologycliniccompatibilitymode-131231002715-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Dental Clinics [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesfordentalclinicscompatibilitymode-131231001855-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Infection Control Guidelines for Nutrition Services [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesfornutritionservicescompatibilitymode-131231001435-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Pharmacy [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforpharmacycompatibilitymode-131231001358-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Laundry Services [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforlaundrycompatibilitymode-131231001333-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Ic guidelines for mortuary care [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesformortuarycarecompatibilitymode-131231001305-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














