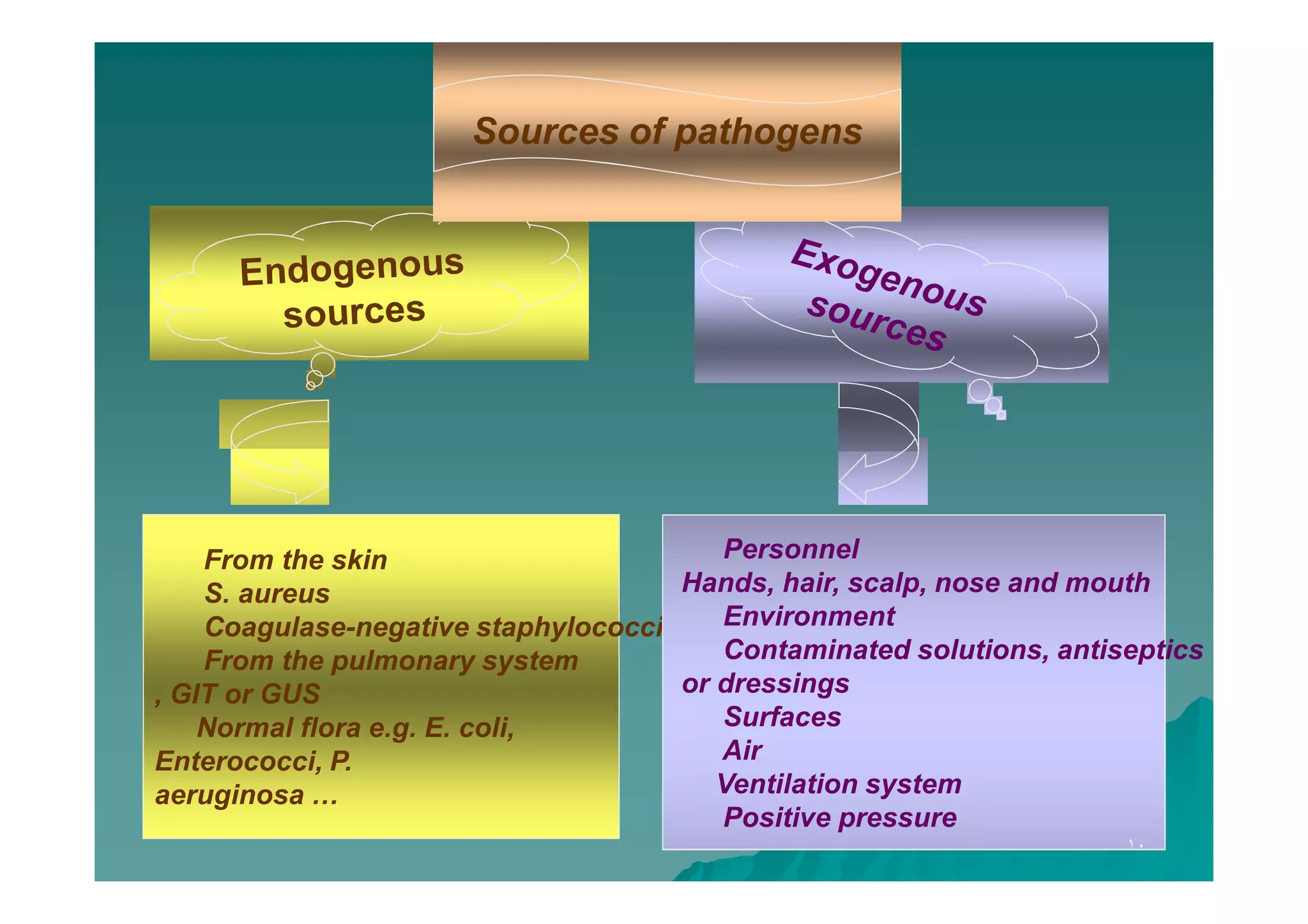
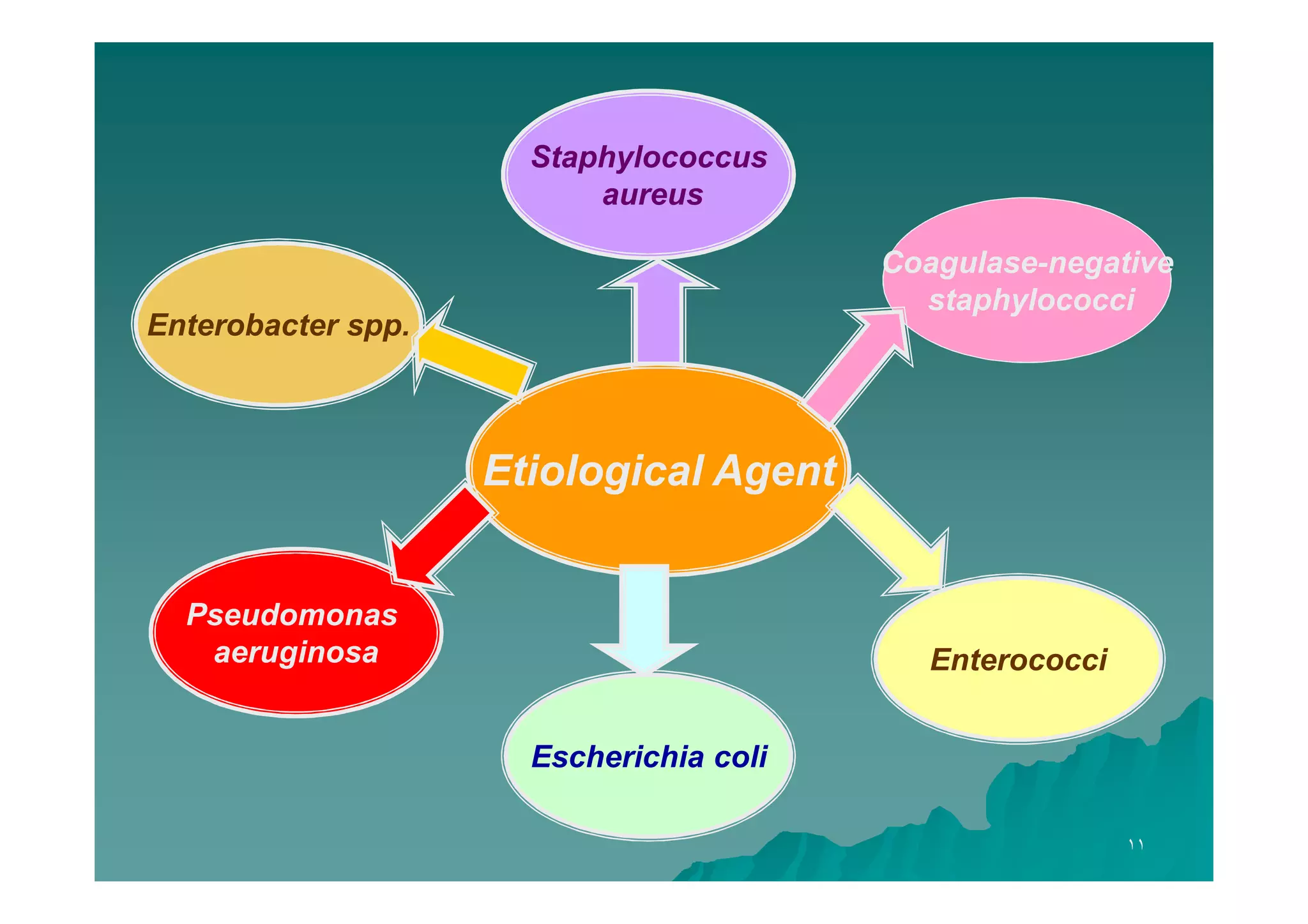
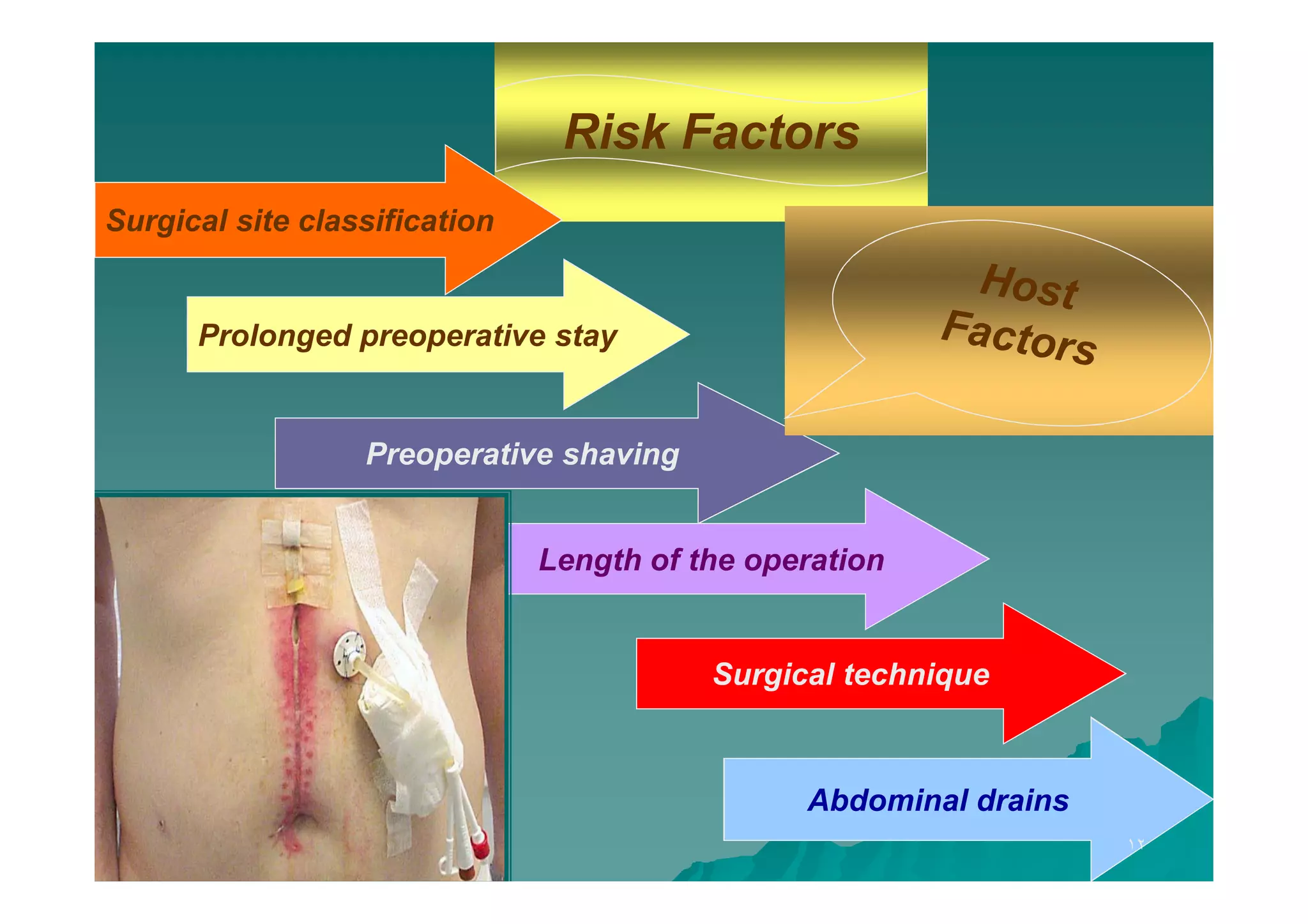
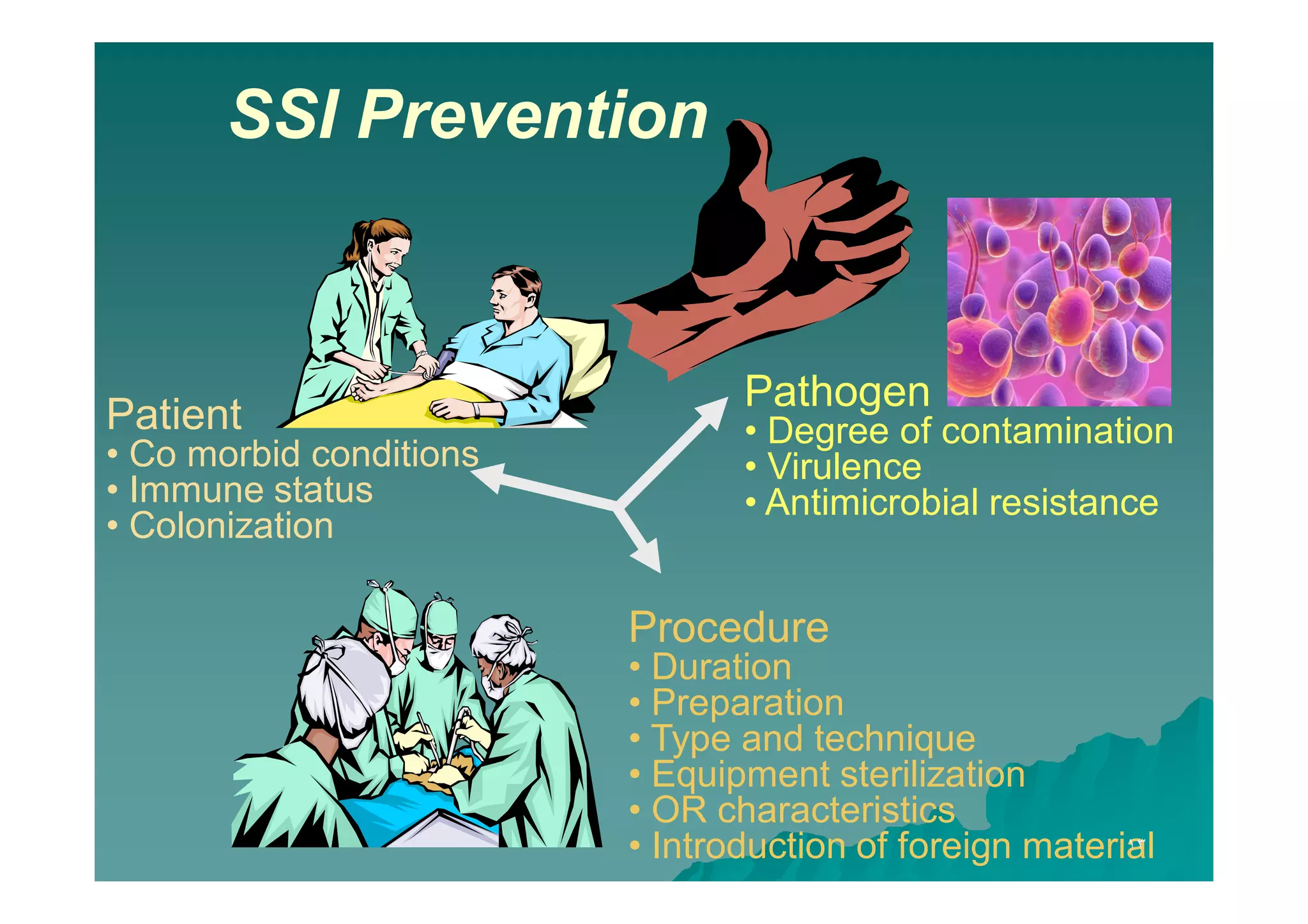
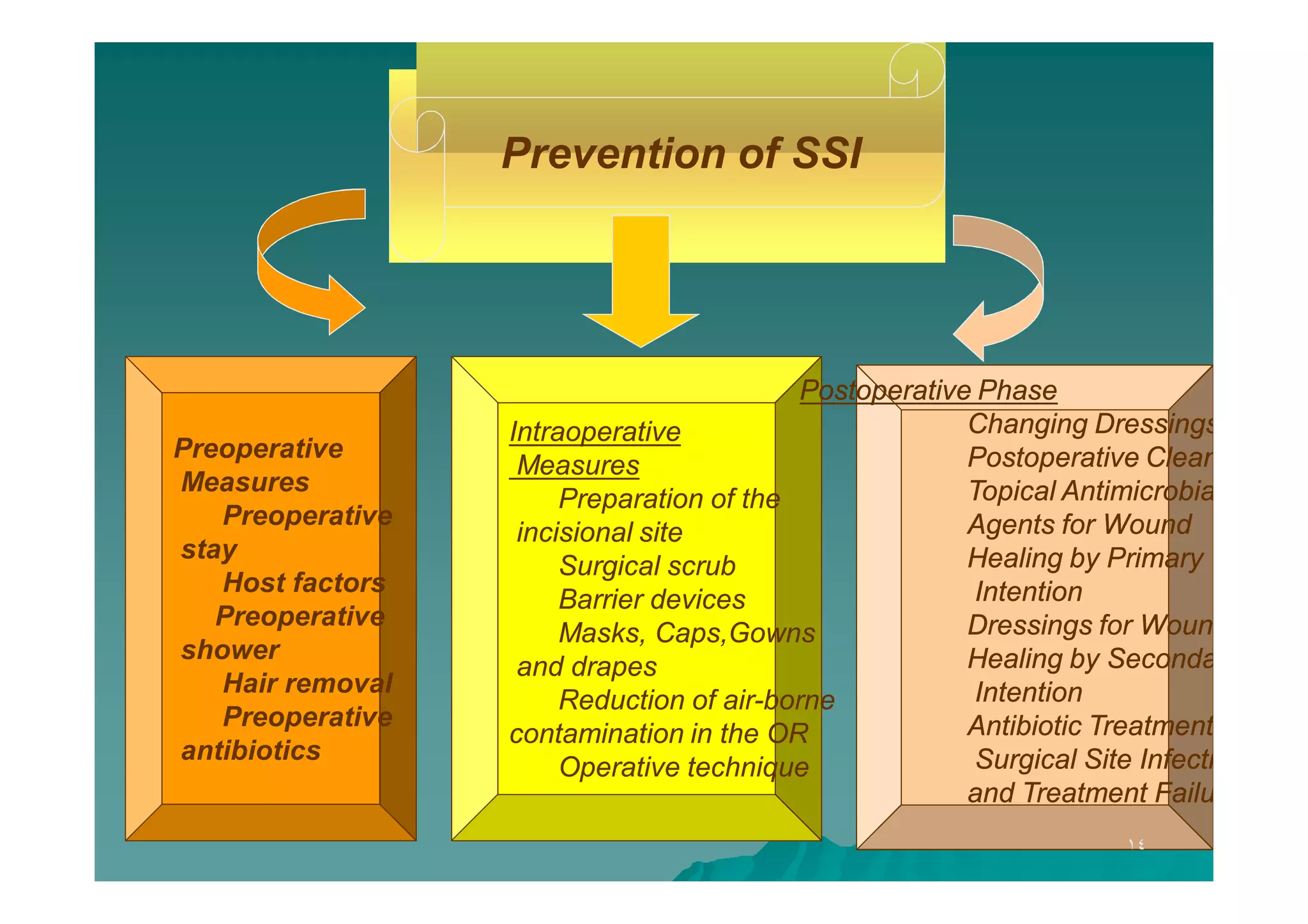
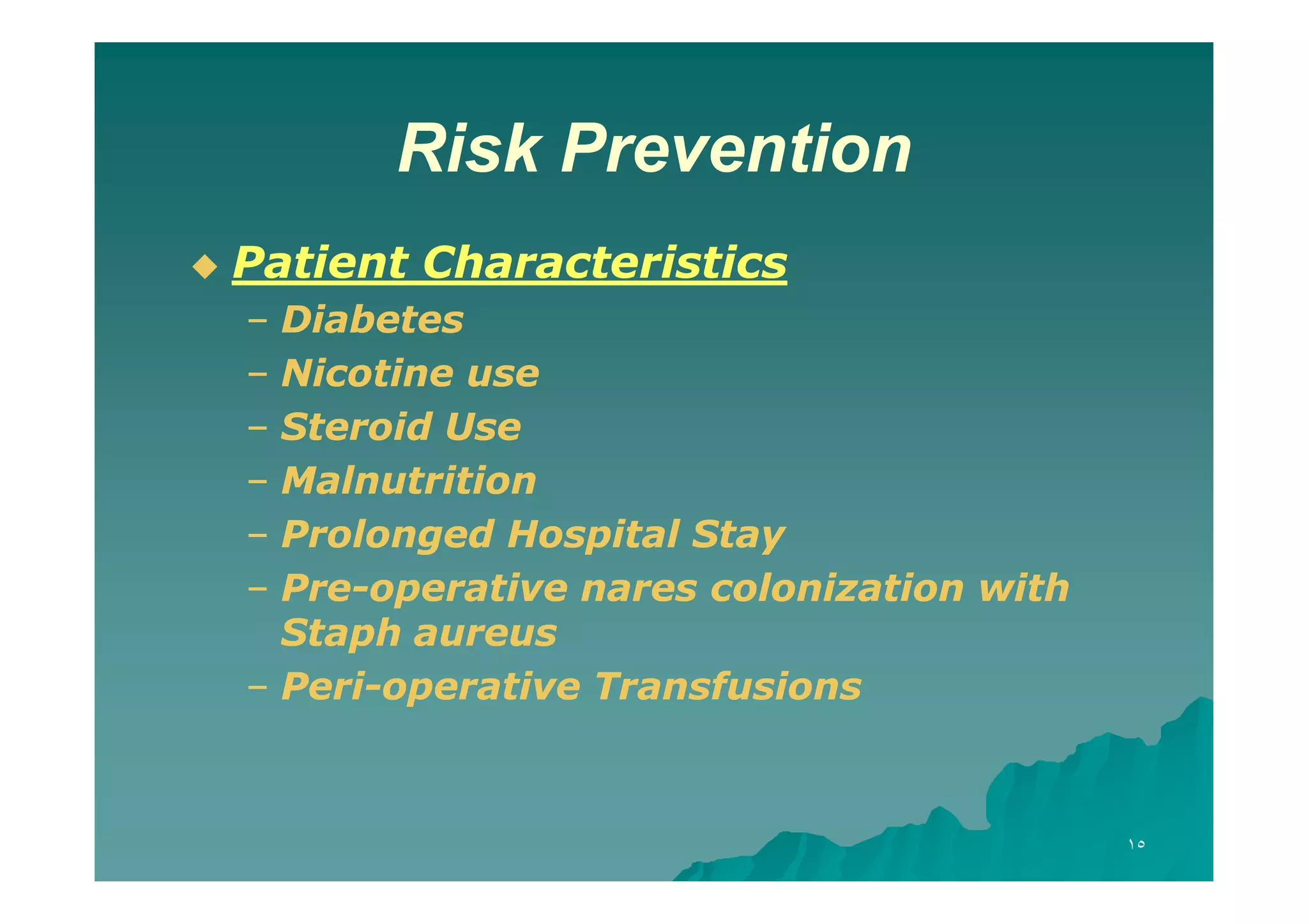
The document discusses the prevalence and impact of surgical site infections (SSI), highlighting their association with increased patient morbidity, mortality, and healthcare costs. It outlines SSI classifications, risk factors, and prevention strategies, emphasizing the importance of proper hygiene, surgical techniques, and antibiotic use before and after surgery. Additionally, it introduces an SSI prevention bundle aimed at optimizing peri-operative care to minimize infection risks and improve patient outcomes.




















![Infection prevention & control general orientation [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/infectionpreventioncontrolgeneralorientationcompatibilitymode-140123020536-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


























































![Role of infection control in patient safety [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/roleofinfectioncontrolinpatientsafetycompatibilitymode-131231012445-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Sharp injuries and needle stick post exposure prophylaxis [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/sharpinjuriesandneedlestickpostexposureprophylaxiscompatibilitymode-131231013025-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Infection Control Guidelines for Laundry Services [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforlaundrycompatibilitymode-131231001333-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Infection Control Guidelines in Tuberculosis [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/infectioncontrolguidlinesintuberculosiscompatibilitymode-131231005155-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Sharp Injuries Prevention[compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/sharpinjuriespreventioncompatibilitymode-131231014416-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Dental Clinics [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesfordentalclinicscompatibilitymode-131231001855-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Nutrition Services [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesfornutritionservicescompatibilitymode-131231001435-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Pharmacy [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforpharmacycompatibilitymode-131231001358-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Ophthalmology Clinic [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforophthalmologycliniccompatibilitymode-131231002715-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Barrier technique personal protective equipment [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/barriertechnique-personalprotectiveequipmentcompatibilitymode-140123022003-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Barrier technique hand hygiene [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/barriertechnique-handhygienecompatibilitymode-140123021839-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Physiotherapy Services[compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforphysiotherapycompatibilitymode-131231001808-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Employee's' health clinic orientation [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/employeeshealthclinicorientationcompatibilitymode-140123022438-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![التعريف العام نعيادة صحة العاملين [Compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/compatibilitymode-140123021257-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















