Downloaded 122 times








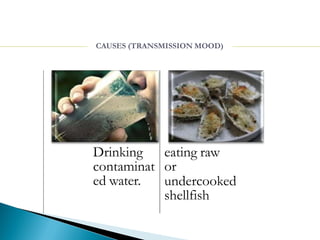



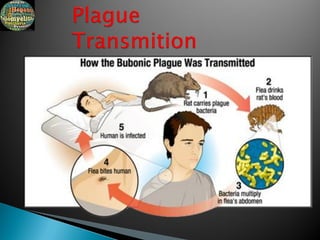





A communicable disease is an infectious disease that is transmitted from one person or animal to another directly or indirectly. Communicable diseases can be transmitted through various modes such as direct contact, droplet infection, contaminated vehicles like food or water, vectors like mosquitoes, and from mother to fetus. Common examples of communicable diseases include respiratory infections like tuberculosis, measles, and influenza; gastrointestinal infections spread through fecal-oral transmission like cholera and typhoid; and vector-borne diseases transmitted by mosquitoes and arthropods.























































































