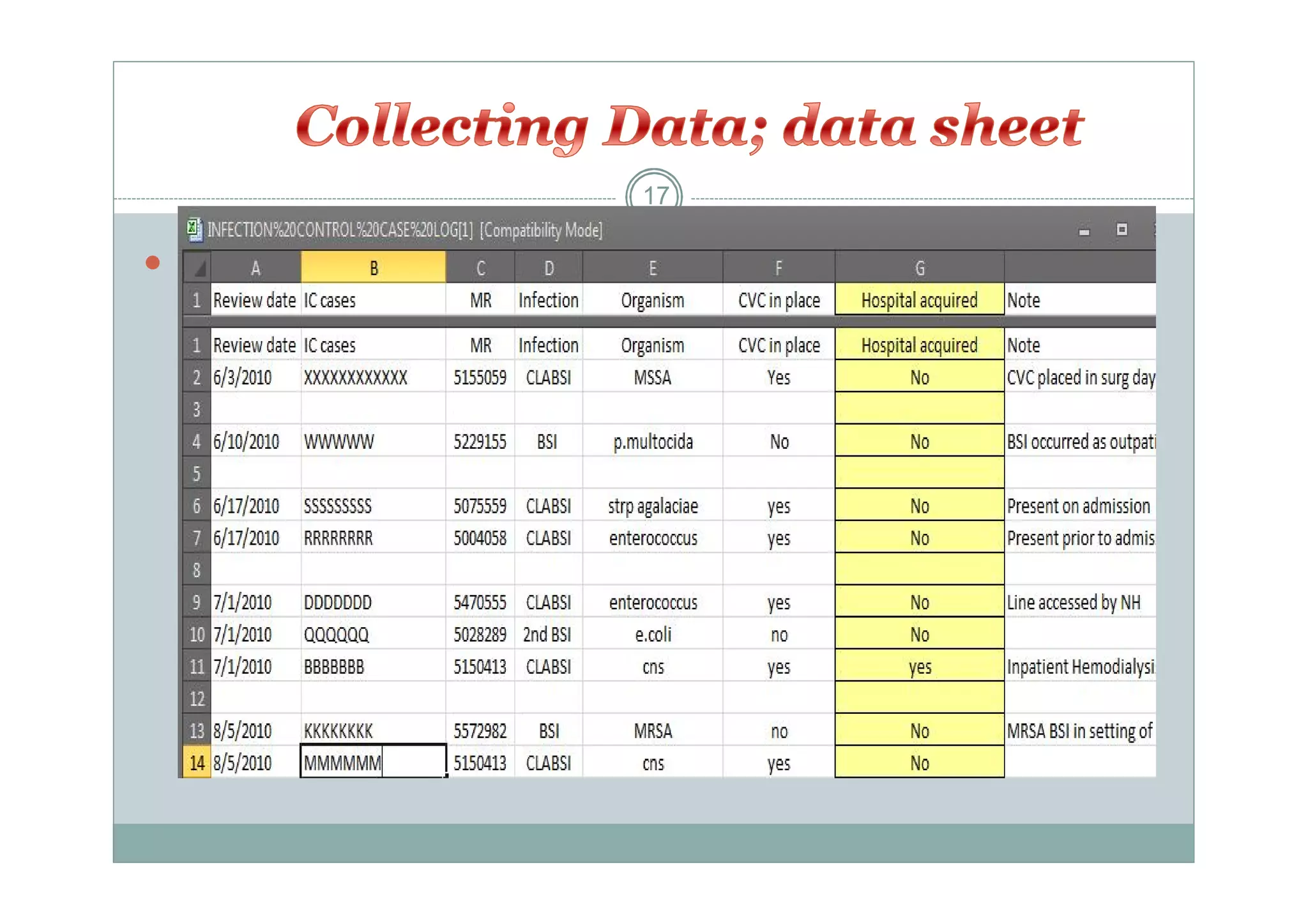
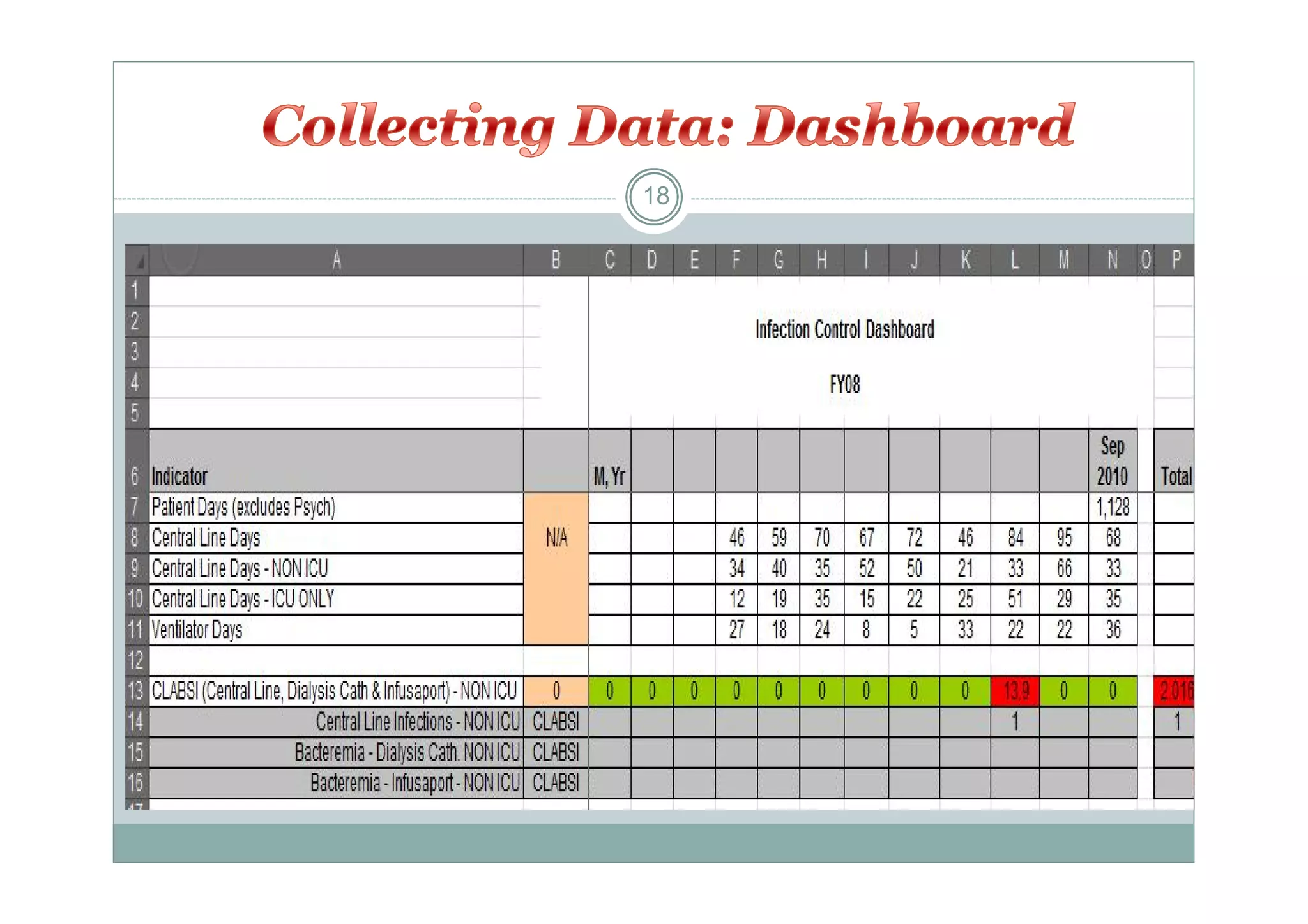
Surveillance involves the systematic and continuous collection and analysis of data for diseases or health conditions in a population. It can be active, involving proactive monitoring approaches, or passive, involving retrospective data review. Surveillance programs typically focus on specific infections, units, pathogens, or procedures based on risk assessments. The goals are to detect outbreaks early, identify prevention opportunities, and disseminate findings to improve health outcomes.
















































![Infection Control Guidelines in Tuberculosis [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/infectioncontrolguidlinesintuberculosiscompatibilitymode-131231005155-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Role of infection control in patient safety [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/roleofinfectioncontrolinpatientsafetycompatibilitymode-131231012445-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection prevention & control general orientation [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/infectionpreventioncontrolgeneralorientationcompatibilitymode-140123020536-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Prevention of Surgical Site Infection- SSI [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/preventionofssicompatibilitymode-131231011316-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Pharmacy [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforpharmacycompatibilitymode-131231001358-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Sharp injuries and needle stick post exposure prophylaxis [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/sharpinjuriesandneedlestickpostexposureprophylaxiscompatibilitymode-131231013025-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Physiotherapy Services[compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforphysiotherapycompatibilitymode-131231001808-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Infection Control Guidelines for Nutrition Services [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesfornutritionservicescompatibilitymode-131231001435-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Sharp Injuries Prevention[compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/sharpinjuriespreventioncompatibilitymode-131231014416-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

![Infection Control Guidelines for Ophthalmology Clinic [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesforophthalmologycliniccompatibilitymode-131231002715-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Barrier technique personal protective equipment [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/barriertechnique-personalprotectiveequipmentcompatibilitymode-140123022003-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Barrier technique hand hygiene [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/barriertechnique-handhygienecompatibilitymode-140123021839-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Employee's' health clinic orientation [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/employeeshealthclinicorientationcompatibilitymode-140123022438-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

![Infection Control Guidelines for Dental Clinics [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/icguidelinesfordentalclinicscompatibilitymode-131231001855-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![التعريف العام نعيادة صحة العاملين [Compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/compatibilitymode-140123021257-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















