

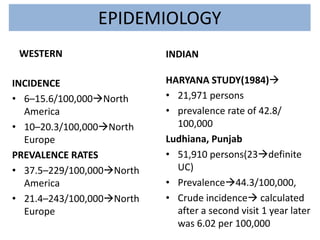
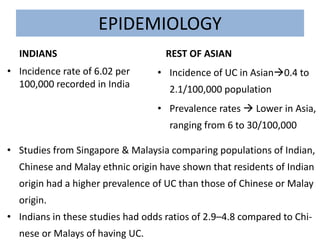
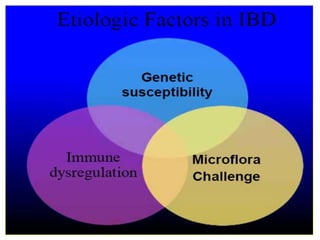
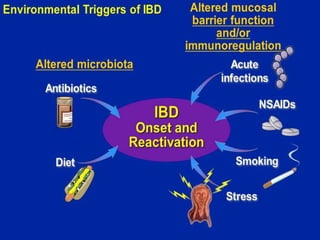
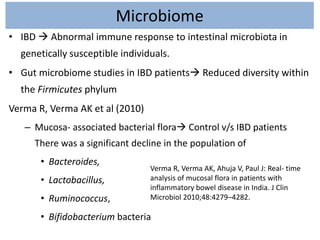
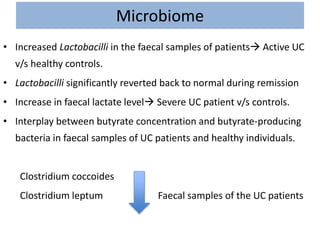




1) Ulcerative colitis is a chronic inflammatory bowel disease characterized by inflammation of the colonic mucosa. It has higher rates in Western countries compared to Asia. 2) Genetic factors play a role in ulcerative colitis, as seen by higher familial risk and specific gene variants conferring increased risk. Environmental factors like smoking and diet also influence disease risk and activity. 3) The microbiome of ulcerative colitis patients shows reduced diversity and changes in populations of bacterial species like Bacteroides and Lactobacillus compared to healthy individuals. Certain genetic syndromes are also associated with higher rates of inflammatory bowel disease.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



