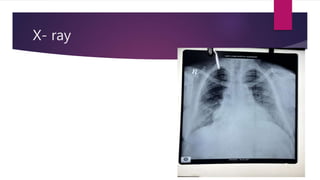
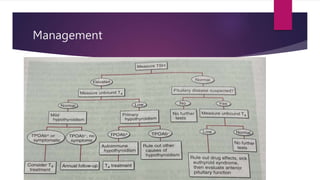
This document presents a case study of a 34-year-old woman with hypothyroidism. Her symptoms include fatigue, blurred vision, vertigo, cold intolerance, menorrhagia, and constipation. On examination, she appears thin, pale, and has delayed reflexes. Laboratory tests show elevated TSH and low T3 and T4, confirming hypothyroidism. Ultrasound reveals an enlarged liver and thyroid nodule. The document then discusses hypothyroidism, its causes, clinical manifestations, diagnosis, and management, including the use of levothyroxine treatment and monitoring of TSH levels. It also covers special populations like pregnant women, the elderly, and cases of myxedema