

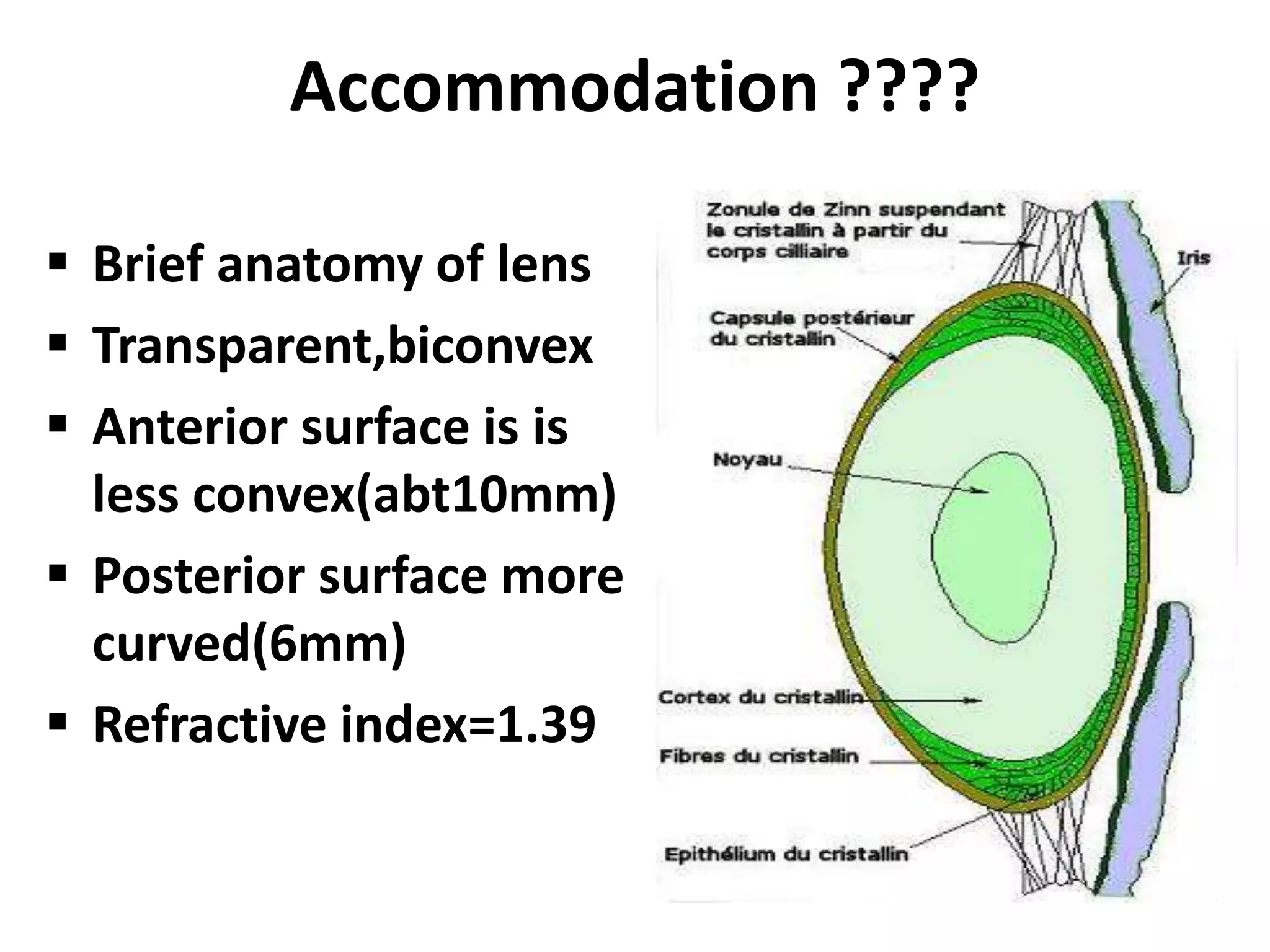
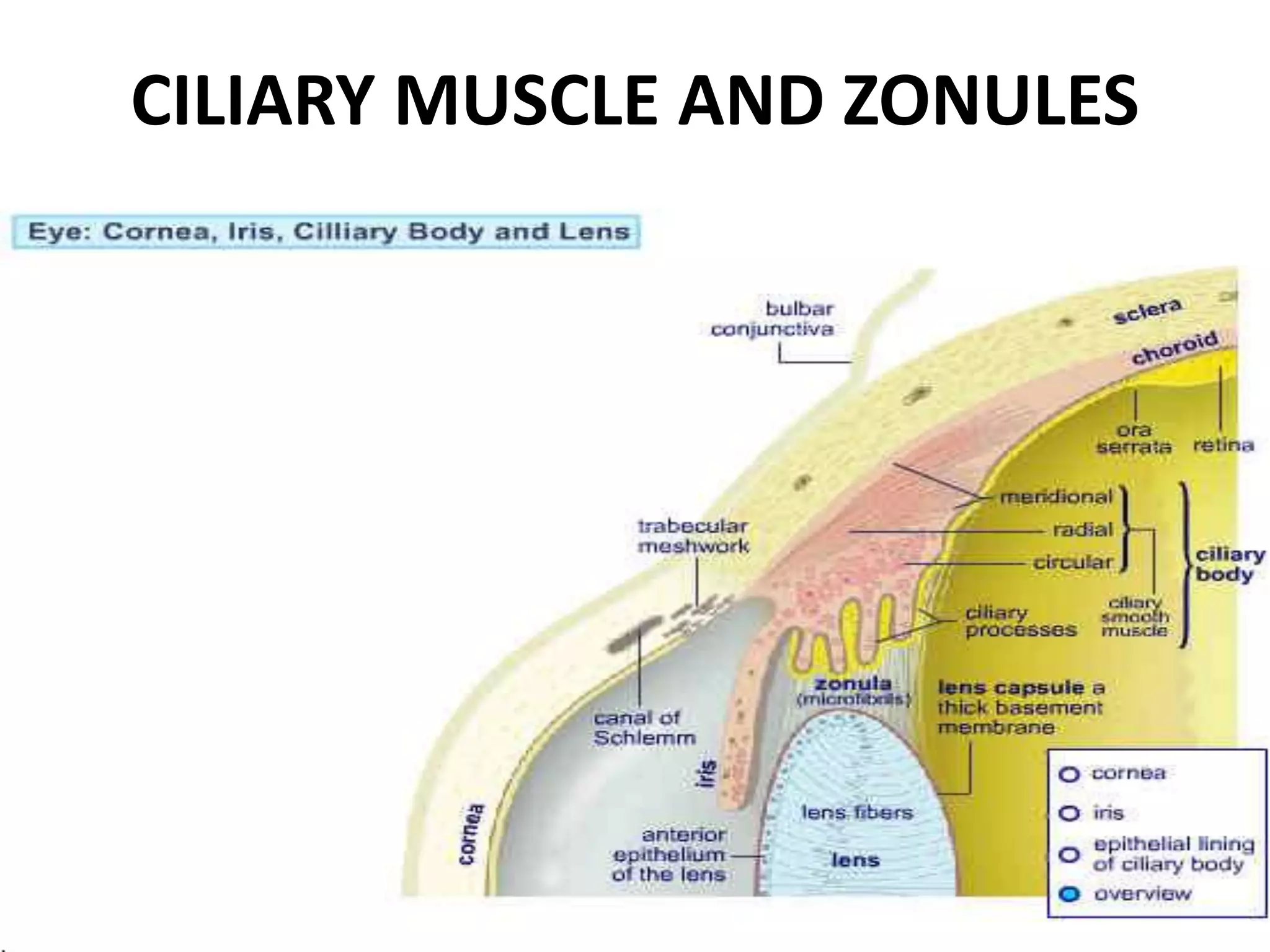



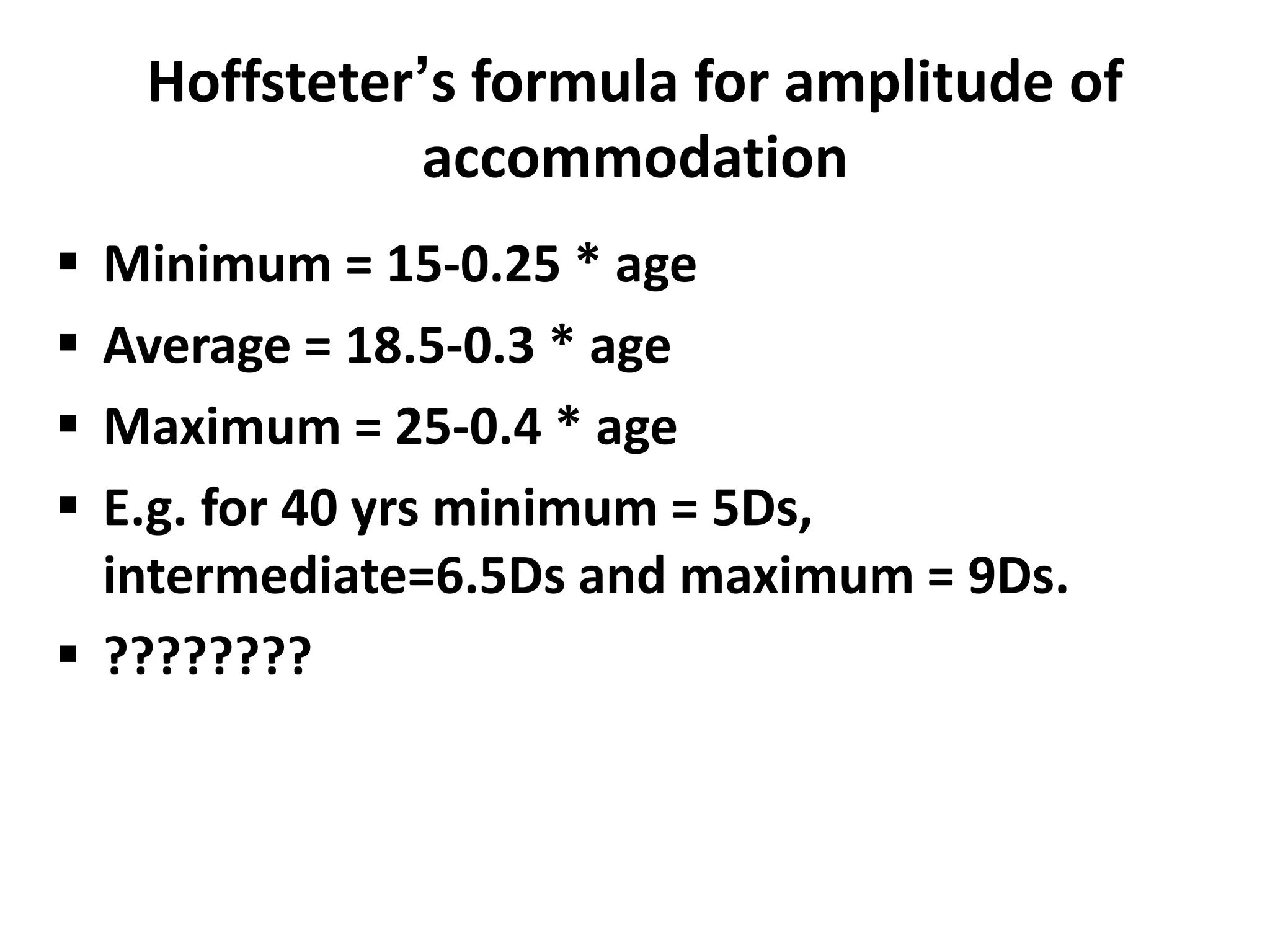





























The document discusses accommodative anomalies and their assessment and management. It begins with an overview of accommodation and the anatomy involved. It then covers topics like the ranges and amplitudes of accommodation and how they vary with age. It discusses various types of accommodative insufficiencies including presbyopia and its correction. It also covers accommodative excess and anomalies like unequal accommodation and accommodative esotropia. Assessment techniques like dynamic retinoscopy and accommodative therapy are described. The document concludes with references for further reading.




















































































