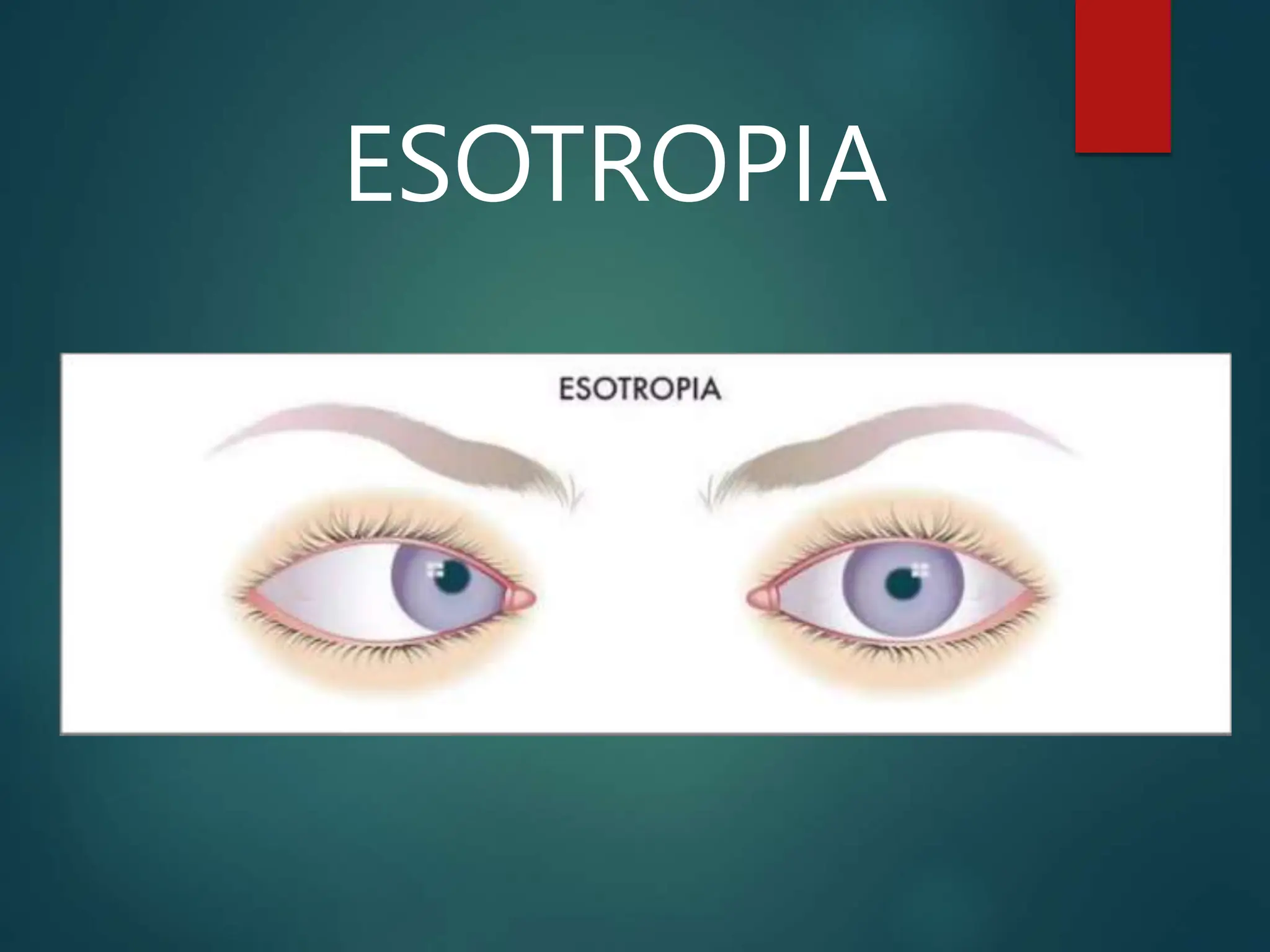
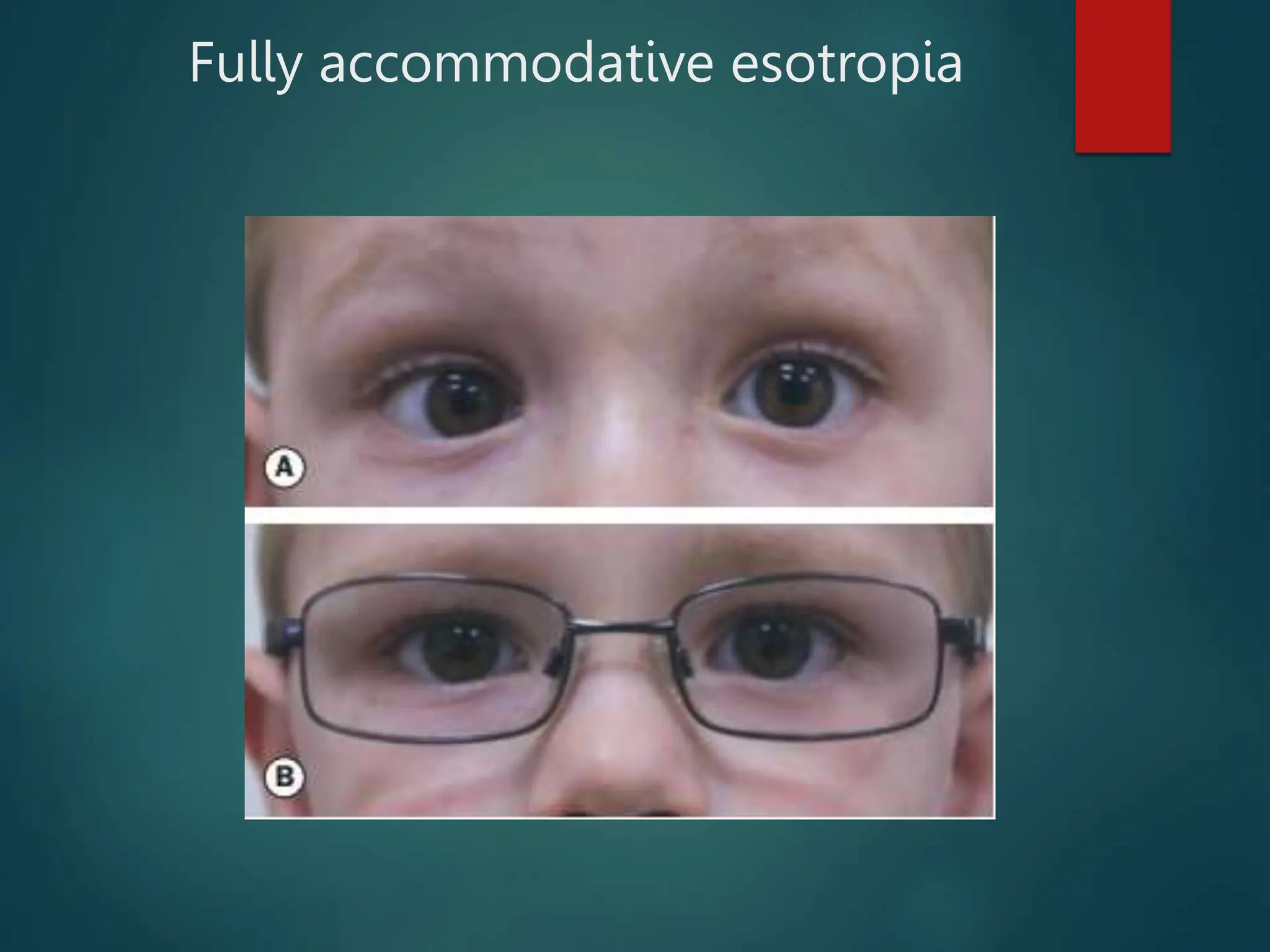
This document provides an overview of esotropia, including its types, causes, and clinical features. Esotropia is a convergent misalignment of the eyes. There are two main types - infantile esotropia, which presents in the first 6 months of life, and accommodative esotropia, which is usually caused by hyperopia. Accommodative esotropia can be fully, partially, or non-refractive. Clinical assessment of esotropia involves measuring visual acuity and the angle of deviation using tests such as cover-uncover and prism cover tests. Treatment involves correcting refractive errors with glasses and potentially strabismus surgery.