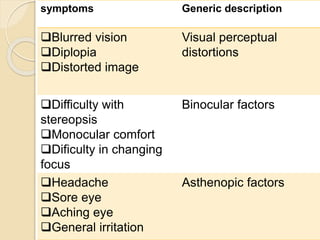
Heterophoria is a latent eye misalignment where the eyes are directed at the fixation point but tend to deviate when fusion is interrupted. It is classified based on direction of deviation (esophoria, exophoria, hyperphoria, cyclophoria) and symptoms (compensated vs decompensated). Esophoria involves a nasal deviation, exophoria a divergent deviation, and hyperphoria/hypophoria an upward/downward deviation of one eye. Compensated heterophoria causes no symptoms while decompensated heterophoria occurs when the deviation cannot be controlled due to weak fusion, leading to issues like blurred vision, diplopia,







































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)