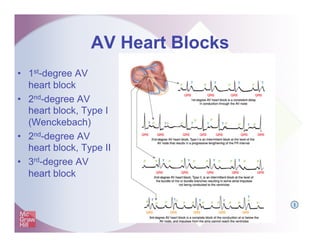
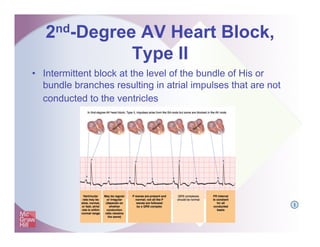
This document discusses different types of atrioventricular (AV) heart blocks. It defines heart blocks as delays or interruptions in conduction between the atria and ventricles. It then proceeds to describe the characteristics of 1st-degree AV block, 2nd-degree AV block types I and II, and 3rd-degree AV block. Specifically, it notes that 2nd-degree type I block shows a regularly irregular rhythm with a progressively lengthening PR interval, while 2nd-degree type II block maintains a constant PR interval with more P waves than QRS complexes. 3rd-degree block results in independent atrial and ventricular rhythms that can decrease cardiac output if the ventricular rate is too slow.

































![Shadechapter09.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter09-150421103043-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter11.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter11-150421103622-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter05.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter05-150421102328-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter14.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter14-150421104301-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter10.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter10-150421103304-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter08.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter08-150421102734-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter13.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter13-150421104054-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)





![Shadechapter07.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter07-150421102520-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)

![Shadechapter15.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter15-150421104606-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)






![ECG & Heart block [doctors online]](https://cdn.slidesharecdn.com/ss_thumbnails/ecgheartblockdoctorsonline-131111054313-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



![Shadechapter02.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter02-150421101545-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Shadechapter03.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter03-150421101919-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)








































