Downloaded 84 times
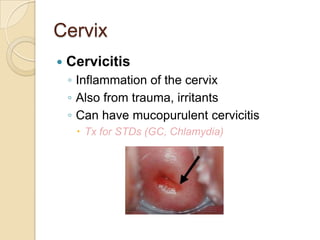
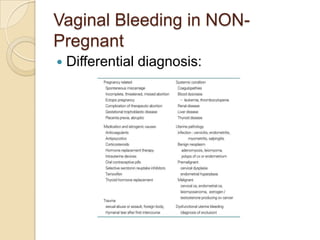
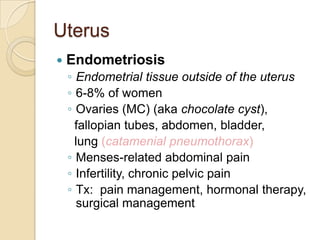
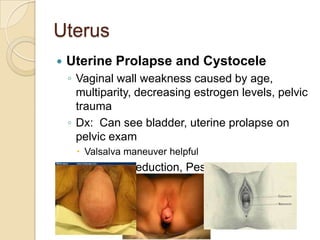
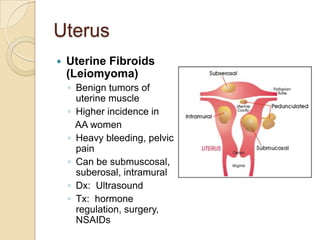



This document provides an overview of common gynecologic disorders organized by anatomy. It discusses conditions affecting the cervix like cervicitis and tumors. For the vagina, it covers issues like Bartholin's abscess, vaginitis, and vulvovaginitis. The uterus section details dysfunctional bleeding, endometriosis, prolapse, and tumors. It also reviews ovarian cysts, torsion, and cancer. Other topics include pelvic inflammatory disease, Fitz-Hugh-Curtis syndrome, gestational trophoblastic disease, and cervical cancer. Clinical presentations, risk factors, diagnoses, and treatments are summarized for each condition.











































































































