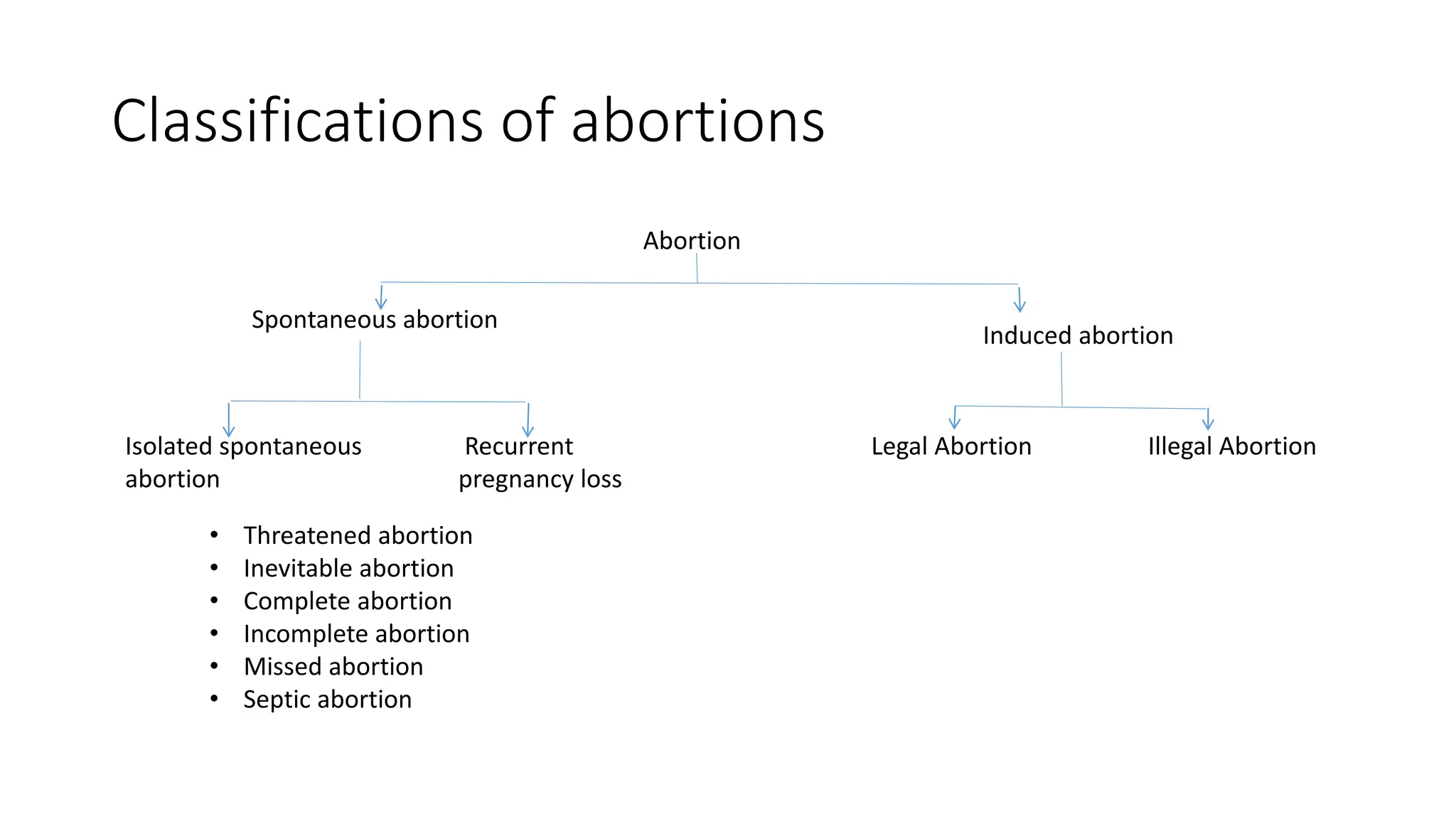
The document provides a comprehensive overview of abortion, covering definitions, classifications, risk factors, and types, as well as management protocols for various abortion instances. It details complications and recurrent pregnancy loss, outlining diagnostic criteria and treatment options for specific conditions like cervical incompetence and apla syndrome. Additionally, it includes guidelines for medical termination of pregnancy (MTP) in India, including consent requirements and methods for performing abortions.