Download as PDF, PPTX



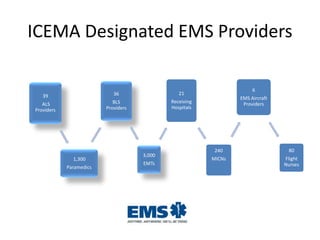

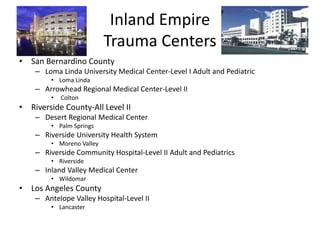
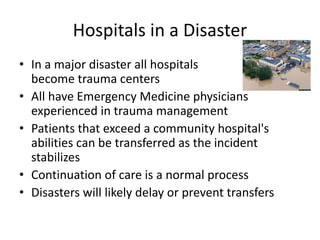
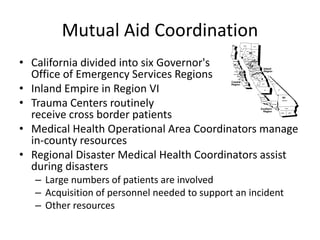



The Inland Counties Emergency Medical Agency (ICEMA) is responsible for coordinating emergency medical services and trauma care across San Bernardino and Riverside counties. ICEMA designates trauma centers, hospitals, and EMS providers and ensures an effective emergency response system. During disasters, all hospitals may receive trauma patients through medical mutual aid agreements within and across counties and states. Trauma centers play an important role but the system is scalable to handle surge from any size incident.











![Organizational Structure Of A Hospital[1]](https://cdn.slidesharecdn.com/ss_thumbnails/organizationalstructureofahospital1-100104091259-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)









































































