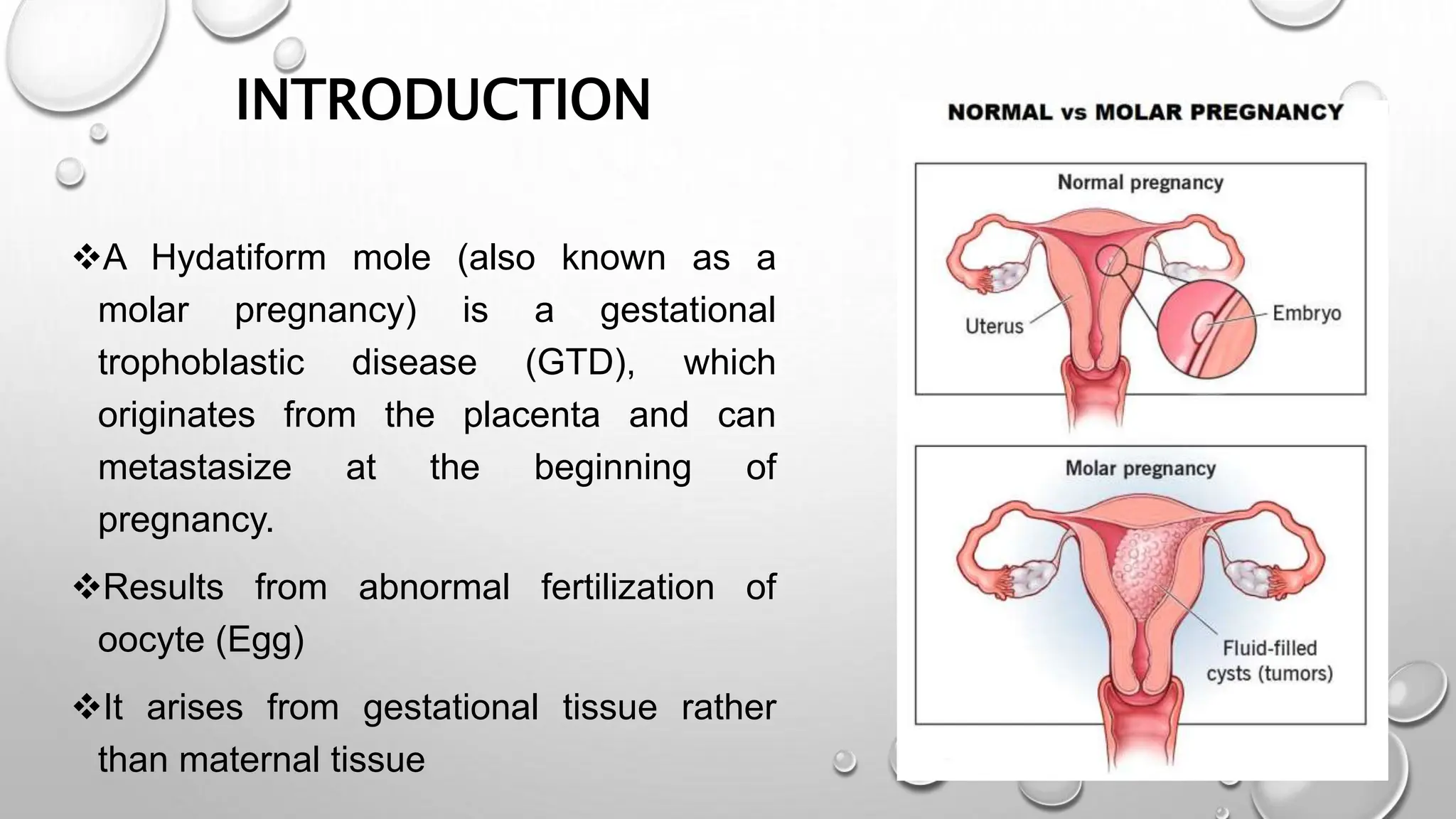
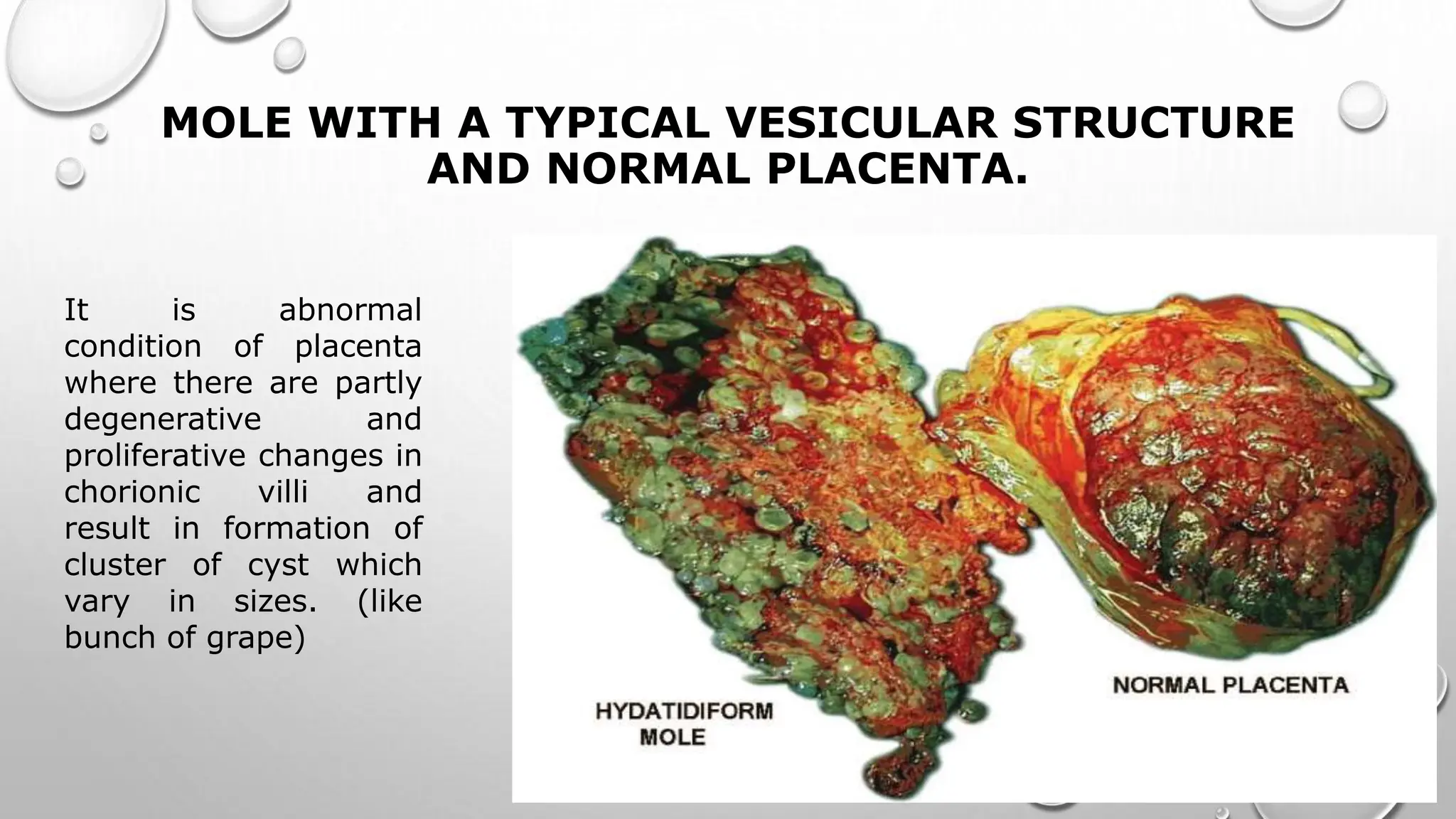
A hydatidiform mole is a gestational trophoblastic disease originating from abnormal placental tissue that can become malignant. There are two types - complete and partial moles. Complete moles are usually diploid and result from fertilization by two sperm or a haploid sperm, while partial moles are usually triploid arising from a normal sperm fertilizing a haploid egg. Clinical features include vaginal bleeding, nausea/vomiting, and high hCG levels. Diagnosis is made through ultrasound and hCG levels. Treatment is surgical evacuation followed by chemotherapy if hCG levels do not normalize or rise. Close follow up is needed to monitor for choriocarcinoma.