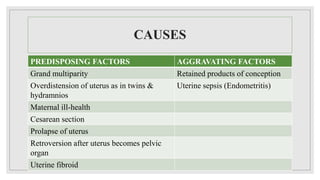
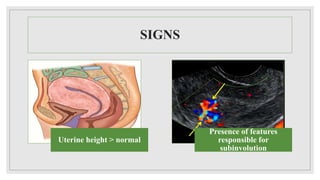
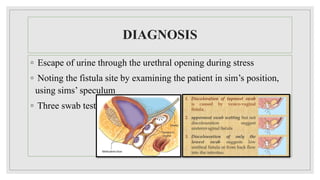



This document discusses subinvolution and urinary tract infections during the postpartum period. Subinvolution occurs when the uterus takes longer than normal to return to its non-pregnant size after delivery and can be caused by factors like multiparity, infection, or cesarean section. Common urinary complications include urinary tract infection, retention of urine, incontinence, and acute kidney injury. Urinary tract infections are treated with antibiotics, fluids, and rest while retention requires catheterization. Acute kidney injury involves phases of oliguria, anuria, early and late diuresis, and recovery managed through fluid balance, nutrition, and dialysis if needed.