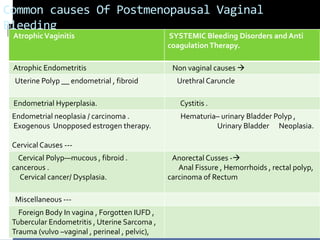
This document discusses common causes and approaches to evaluating and managing postmenopausal vaginal bleeding. Key causes mentioned include atrophic vaginitis, endometrial hyperplasia, uterine polyps, endometrial cancer, and exogenous estrogen use. The diagnostic approach involves a detailed history, examination, transvaginal ultrasound, hysteroscopy, and biopsy. Initial stabilization priorities bleeding control. Long-term management depends on the underlying cause and may involve hormone therapy, surgery, or chemotherapy/radiotherapy. Counseling supports informed decision making and long-term follow up.