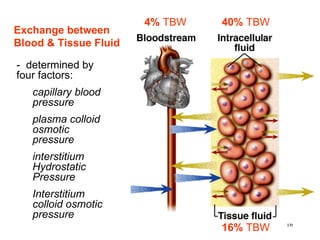
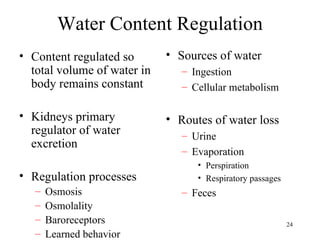

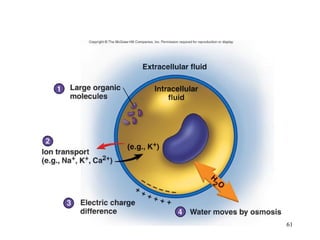

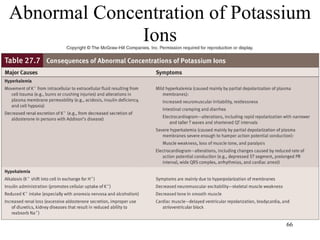
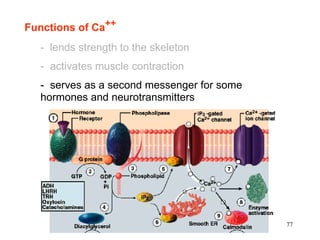
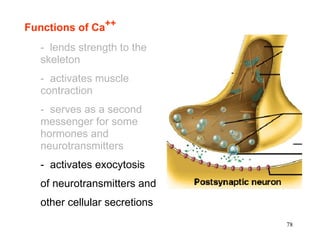
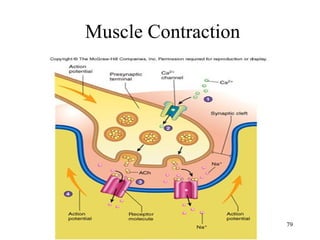
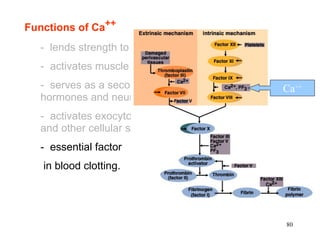
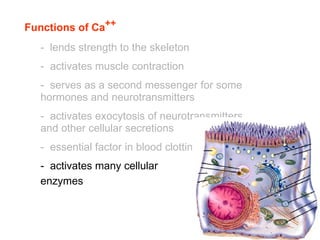
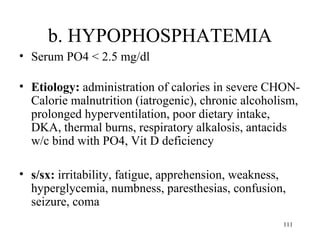
![Functions of Ca++
- lends strength to the skeleton
- activates muscle contraction
++
Excitation [ Ca ]i Contraction
(Action Potentials) (shortening)
76](https://image.slidesharecdn.com/ncm103aug22fluidsandelectrolyte-120609024036-phpapp01/85/Fluids-Electrolyte-76-320.jpg)
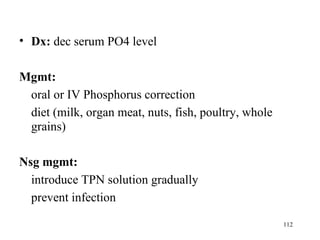
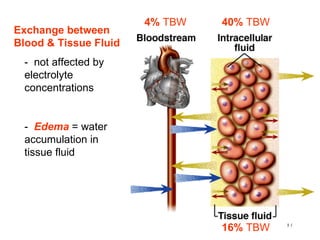
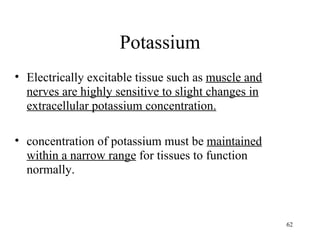
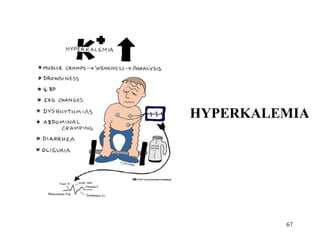
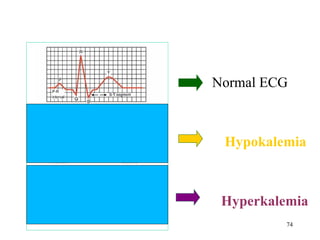
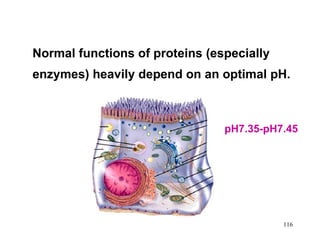
![pH
is the negative logarithm of H+
concentration, and an indicator of acidity.
pH = - log [H+ ]
Example: [H+ ] = 0.1 µM = 10 –7 M
115](https://image.slidesharecdn.com/ncm103aug22fluidsandelectrolyte-120609024036-phpapp01/85/Fluids-Electrolyte-115-320.jpg)

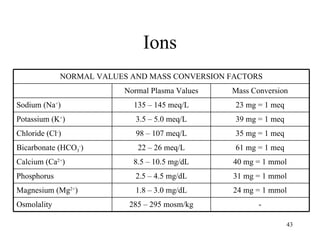
- Monitor VS, LOC, I and O, weight - Monitor Na levels closely - Seizure precautions - Oral care - Initiate feedings slowly - Educate on fluid restriction - Identify and treat underlying cause Prevent rapid correction to avoid osmotic demyelination syndrome 58 Potassium - Most abundant intracellular cation - 3.5-5.0 mEq/L - Regulated by: - Dietary intake - Renal excretion - Shift between intra/extracellular space Functions: - Important in nerve impulse conduction - Muscle contraction - Acid-base balance - Glucose metabolism





























































































![Getting Started with Apache Spark: Big Data Made Simple [Free Meetup]](https://cdn.slidesharecdn.com/ss_thumbnails/apachesparkgettingstarted-260203175547-8361bcc3-thumbnail.jpg?width=640&height=640&fit=bounds)











