Lithium is a mood stabilizer used to treat bipolar disorder. It works by altering sodium transmission in nerves and modulating neurotransmitter levels in the brain.
Psychotherapeutic Agents
1. Whatdoes it mean when a drug has a sedative
effect?
2. What is the difference between sedation and
hypnosis?
3. What are the level of anxiety?
2
3.
States Affected bySedative-
Hypnotics
1. Anxiety
– Feeling of tension, nervousness or apprehension
– Manifested associated with SYMPATHETIC NS
• Sweating, fast heart rate, rapid breathing and elevated BP
– Mild
• Lowest level, source of positive motivation in certain situation
– Moderate
– High
• Overwhelming, can cause interference with activities of daily living
3
4.
States Affected bySedative-Hypnotics
2. Sedation
– loss of awareness and reaction to environmental stimuli
– Diminished physical & mental response
– Drugs can be administered to sedate client
• Irritable and restless
4
5.
States Affected bySedative-Hypnotics
3. Hypnosis
– Extreme state of sedation in which the person
no longer sense or reacts to incoming stimuli
– Effective hypnotics act on the RAS and block
the brain’s response to incoming stimuli
5
Benzodiazepines
Action:
• Act onlimbic system and RAS to enhance the action of gamma-
aminobutyric acid (GABA)
• GABA = inhibitory neurotransmitter
– depress neuronal function at multiple sites in the CNS
– Also promote sleep by affecting cortical areas and sleep-wakefulness cycle
– Muscle relaxation thru effects on supraspinal motor areas =cerebellum
8
9.
Benzodiazepines
Indications:
• Drug ofchoice for anxiety and insomnia
• Anxiety disorders
• Alcohol withdrawal
• Hyperexcitability & agitation
• Short-acting are administered through IM
– Preop to sedate the client
– Before short diagnostic procedures
– For induction of general anesthesia
9
Barbiturates
Actions:
• Bind withGABA receptors to enhance inhibitory functions
• Are general CNS depressants that inhibit neuronal
impulse conduction in ascending RAS
• Depress cerebral cortex
• Alter cerebellar function and depress motor output
16
17.
Barbiturates
Indications:
• LONG ACTING(phenobarbital & mephobarbital)
– Control seizures in epilepsy
• INTERMEDIATE ACTING (amobarbital, aprobarbital)
– Use in maintaining long periods of sleep
• SHORT-ACTING (thiopental sodium)
– Used as general anesthetic
17
Barbiturates
Adverse Effects:
• Withincreasing dosage, responses range from sedation – sleep –
general anesthesia
• Can ↓BP & HR; toxic dose lead to shock
• They stimulate hepatic enzymes that can accelerate their own
metabolism and that of other drugs
• Prolonged used=physical dependence
20
21.
Sedative-Hypnotic Drugs
General NursingConsiderations:
• Do not administer intra-arterially
– Serious arteriospasm and gangrene can occur
• Do not mix IV drugs in solution with other drugs
– To avoid drug-drug interxn
• Parenteral forms should be the last resort, only if oral forms are
not available
– Oral less likely cause AE
• Give IV medications slowly
– Rapid administration can cause cardiac problems
21
22.
Sedative-Hypnotic Drugs
General NursingConsiderations:
• Maintain client who receive parenteral benzodiazepines in bed
for a period of 3 hrs
• Monitor hepatic & renal functions, CBC during long therapy
• Taper dosage gradually after long-term therapy, esp in epileptic
client
– Abrupt withdrawal could trigger seizures
22
23.
Sedative-Hypnotic Drugs
General NursingConsiderations:
• Prepare emergency life support facilities in case of
severe respiratory depression
• Provide comfort measures to help client tolerate drug
effects
– Small, frequent meal
– Consume drug with food
23
Major Depression Disorder
•Characterized by:
– Low mood
– Low self-esteem
– Loss of interest or pleasure in normally
enjoyable activities
• Commit suicide
25
26.
Biogenic Amine Theoryof Depression
• Depression results from a deficiency in biogenic amines:
– norepinephrine, dopamine and serotonin
• Norepinephrine
– Alertness & energy, anxiety, attention and interest in life
• Serotonin
– Anxiety, obsession and compulsion
• Dopamine
– Attention, motivation, pleasure and reward and interest in life
26
27.
Biogenic Amine Theoryof Depression
• Deficiency of these neurotransmitter may be caused by:
– Breakdown by monoamine oxidase to be recycled or restored in
neuron
– Rapid or sudden abnormal electrical discharges from the brain
– Increase in # or sensitivity of postsynaptic receptors
27
28.
Anti-Depressant Drugs
• Givenwith major depression
• Works: balance the neurotransmitters
• Purpose:
– Improve sleeping pattern
• Onset/effective:
– 2-3wks after
– Given with anti-psychotic to minimize bizarre behavior
– On 3rd week:
• Very watchful and vigilant
• Pt can commit suicide
– Have enough energy
28
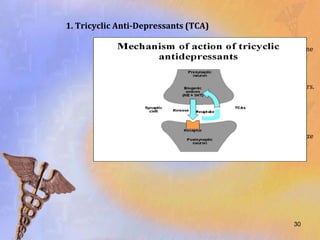
1. Tricyclic Anti-Depressants(TCA)
• TCAs inhibit uptake at presynaptic junction of the norepinephrine
and serotonin
• results in the accumulation of these neurotransmitter in the
synaptic cleft and increased stimulation of postsynaptic receptors.
• asserts that depression stems from a deficiency in monoamine-
mediated transmission.
• Elevate mood, increase alertness, improve appetite and normalize
sleep patterns.
30
31.
1. Tricyclic Anti-Depressants(TCA)
• Preferred drug for major depression.
• Therapeutic effect: 1-3 wks
• Full relief of symptoms: 1-2mos
• Tx of enuresis in children >6yo due to its anticholinergic
effects
31
1. Tricyclic Anti-Depressants(TCA)
Contraindications:
• Recent MI
– Reinfarction can occur
• Undergone myelography within prev 24h or in the next
24h
• Should not be taken with MAOI
– Severe HYPERPYRETIC CRISIS with severe convulsion
– Elevated BP and death
33
34.
1. Tricyclic Anti-Depressants(TCA)
Caution:
• With cardiovascular disorders
• Hx of seizures
– Seizure threshold may decreased
• Renal and liver disease
34
2. Monoamine OxidaseInhibitors
• MAO is an enzyme found in liver, intestinal wall and
terminals of monoamine-containing neurons
• Function:
– convert norepinephrine, serotonin and dopamine into inactive
products
– In intestine, MAO serves to inactivate tyramine and other biogenic
amines in food
38
2. Monoamine OxidaseInhibitors
Action:
• Irreversibly inhibit MAO
• Preventing the inactivation of neurotransmitters.
• Allows accumulation of such chemicals in
postsynaptic receptors
40
2. Monoamine OxidaseInhibitors
Contraindications:
• + allergy to MAOI
• Pheochromocytoma
– Tumor of adrenal gland
– Sudden ↑norepinephrine = HYPERTENSIVE CRISIS
• 1st sign: pounding occipital headache
• Give REGITINE (antidote)
• Cardiovascular dse
• Scheduled for myelography w/in past 24h to next 48h =
reaction to dye
42
43.
2. Monoamine OxidaseInhibitors
Caution:
• Psyche pt = lead to overstimulation/manic
phase
• Seizure disorders & hyperthyroidism =
exacerbate stimulation of drug
43
44.
2. Monoamine OxidaseInhibitors
Adverse Effect
• In contrast to TCA, MAOI cause direct CNS
stimulation
– Excessive stimulation produce:
• anxiety
• Agitation
• Hypo/hypermania
• Orthostatic hypotension
44
45.
MAOI + TYRAMINE
not compatible
Cause HYPERTENSIVE CRISIS
Special Nursing Consideration:
• NO TYRAMINE RICH FOOD
– Processed foods
– Fermented foods
– Preserved foods
– Ex. Use of yeast, cheese, f.sausage, aged fish and meat
– Give WHITE wine & cheese (cottage)
45
3. Selective SerotoninReuptake Inhibitors
(SSRI)
• Block the reuptake of serotonin into the
nerve terminal of the CNS
• Enhancing its transmission at the
serotonergic synapse
47
If pt wantsto get pregnant
To change drug:
Gradual ↓dosage of SSRI to MAOI
Examples of SSRI:
Z
OLOFT
PA IL
PRO AC
52
53.
4. Atypical Antidepressants
•Also called second-generation antidepressants
• Affect 1 or 2 of the 3 neurotransmitters (serotonin, dopamine&
norepinephrine)
• Used in treating depression who do not respond to other
antidepressants
• Examples:
– bupropion (Wellbutrin)
– amoxapine (Asendin)
– nefazodone (Serzone)
53
54.
Anti-Depressants
General Nursing Considerations:
•Maintain initial dosage for 4-8wks to achieve full
therapeutic effect.
• Maintain suicide precaution for severely depressed
clients
• Monitor BP and PR on regular schedule; q4
• Instruct to avoid sudden change in position
– to prevent orthostatic hypotension
• Advise to avoid hazardous activities if sedation is
prominent
54
55.
Anti-Depressants
General Nursing Considerations:
•Encourage to undergo ECG prior and during tx
• Instruct not to abruptly stop taking the drug. Dosage
should be gradually decreased
• Encourage client who wants to get pregnant to consult
HCP about possible teratogenic effects of the drug on
fetus.
55
1. Lithium
Actions:
• Alterssodium transmission in nerve and muscle cells
• Inhibit release of norepinephrine and dopamine but not serotonin
• In manic client, lithium reduces euphoria & hyperactivity
• Antimanic effect begins at 5-7days after onset of tx
• Full benefit: 2-3 wks
58
1. Lithium
• Renalexcretion is affected by blood levels of sodium.
• Lithium excretion is reduced when blood levels of sodium
are low.
• Thus, toxicity happens when there is not enough sodium
in the blood
• Dehydration will cause lithium to remain in
kidneys, accumulation can lead to toxicity
62
1. Lithium
Special NursingConsiderations:
1. Draw samples immediately before the next dose (8-12hrs after
previous dose)
2. Advise to maintain adequate fluid intake
– 2-3L/day initially
– 1-2L/day maintenance
3. advise to maintain adequate Na++ intake and to avoid
crash diets that affect physical and mental health
69
70.
1. Lithium
Special NursingConsiderations:
4. Can be taken with meals
– to decrease gastric irritation
5. Therapeutic effect will be observed after 1-2 weeks
6. Advice client who are planning to conceive to consult with HCP about
possible teratogenic effects on fetus
70
71.
2. Valproic Acid
Action:
•Control symptoms in acute manic episodes
• Can provide prophylaxis against recurrent episodes of mania
and depression
• Has higher therapeutic index than lithium and more desirable
side effects
71
72.
2. Valproic Acid
Action:
•Increases levels of GABA in brain, resulting to decreased
seizure activity
• Starting dosage in adult:
– 250mg, tid
• Maintenance 1000-2500mg/day
72
3. Carbamazepine
• Likelithium, reduces symptoms of manic and depressive
episodes
• Preferred for
– with mixed mania/rapid-cycling bipolar disorder
• For tx of acute manic episodes, dosage increases
• Maximum dosage: 1600-2000mg/day
76
Case Analysis
M.H, 38years old, was started on oral lorazepam for her anxiety attacks.
Four days after, she calls the clinic complaining that the dose must
not be high enough because she reports that her symptoms of anxiety
have been increased. She feels euphoric and excited for no reason and
she has difficulty falling asleep.
a. What is the therapeutic action of lorazepam?
b. What is your assessment of the client’s problem?
c. What will be your nursing interventions at this time?
79