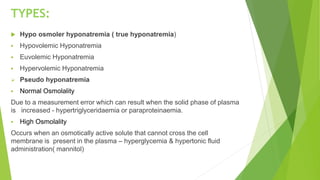
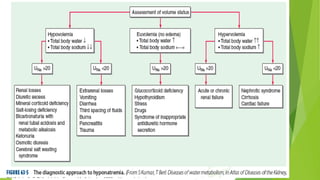
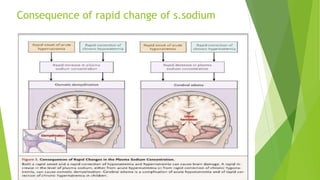
Sodium homeostasis and the regulation of serum sodium concentration is essential for normal physiological functioning. Hyponatremia occurs when there is a relative excess of water compared to sodium, decreasing the plasma sodium concentration below 135 mmol/L. It can be hypo-osmolar, euvolemic, or hypervolemic depending on water and sodium levels. Treatment involves correcting the underlying cause, restricting water intake, and sometimes using hypertonic saline or vaptans. Rapid correction of sodium levels can have neurological consequences, so changes should be gradual. Hypernatremia is less common but also dangerous, defined as a sodium level over 145 mmol/L.