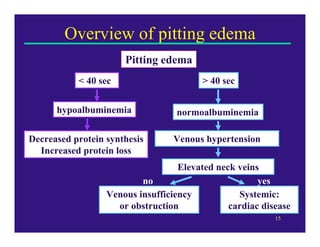
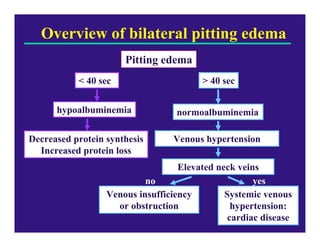
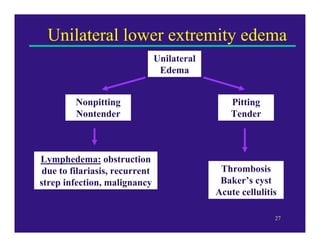
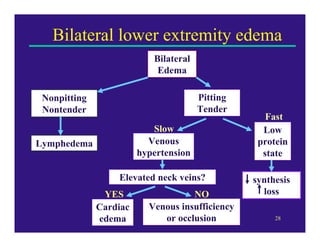
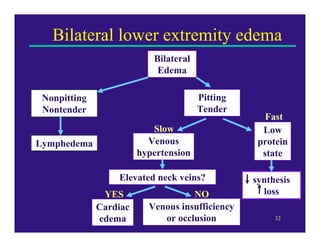
Edema can be caused by increased hydrostatic pressure, decreased plasma oncotic pressure, or lymphatic obstruction. Increased hydrostatic pressure can result from heart failure, liver cirrhosis, or venous obstruction. Decreased plasma oncotic pressure occurs when albumin is lost, such as in nephrotic syndrome, or not produced sufficiently, as in liver disease or malnutrition. Lymphatic obstruction leads to localized edema and can be caused by infection, cancer, or surgery. Edema fluid accumulation in tissues can impair function and be life-threatening in the lungs or brain.