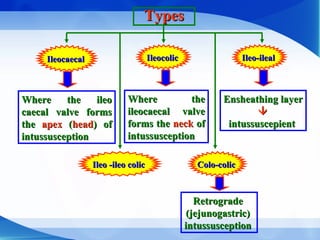
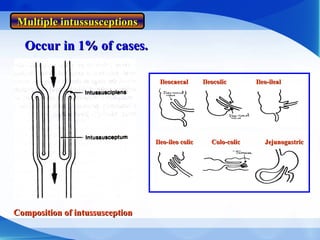
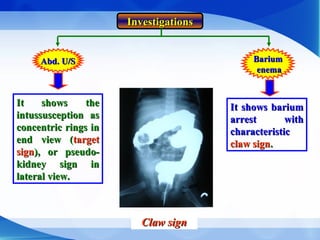
The document discusses intussusception, an invagination of a bowel segment that can lead to partial obstruction, particularly in infants and adults, with symptoms including abdominal pain, vomiting, and the presence of a palpable mass. It outlines the types (idiopathic and organic causes), pathology, complications, clinical presentation, and diagnostic methods such as ultrasound and barium enema, as well as treatment options that include both non-operative and operative reduction techniques. Additionally, it covers volvulus, describing its causes, clinical signs, and treatment strategies.