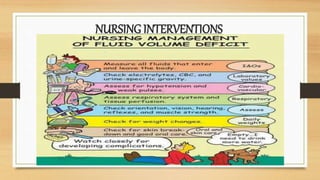
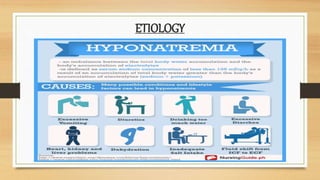
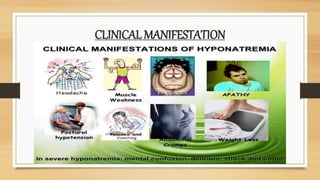
This document discusses various fluid and electrolyte imbalances including their causes, clinical manifestations, treatment, and nursing interventions. It covers fluid volume deficit and excess, as well as electrolyte imbalances involving sodium, potassium, and calcium levels. Fluid volume deficit can result from conditions like diarrhea, vomiting or fever that cause fluid loss. Treatment involves oral or IV fluid replacement depending on severity. Fluid volume excess has causes like congestive heart failure and is treated with diuretics and fluid restriction. Electrolyte imbalances are also discussed including hypocalcemia, hypokalemia, hyponatremia, and hyperkalemia.



![Fluid and electrolyte imbalance [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/btwa8l8ysletobnf0row-signature-f3069b4a7063ad7d39b14083d6e8689bac823dbcf19c3f5cb443fa8d754857b7-poli-171013171124-thumbnail.jpg?width=640&height=640&fit=bounds)
































![WILLIAM__FLUID_AND_ELECTROLYTE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/williamfluidandelectrolyte1-230310182617-481b32fd-thumbnail.jpg?width=640&height=640&fit=bounds)






































