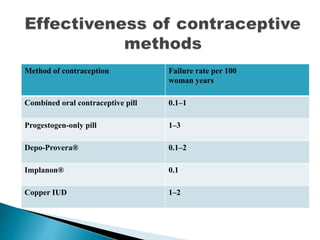
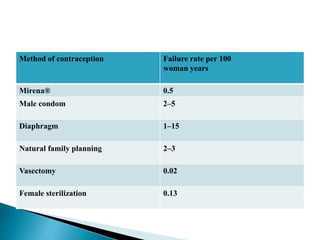
The document discusses various methods of contraception, their effectiveness, side effects, and appropriate usage. It covers hormonal methods like combined oral contraceptives (pills), patches, rings, and progestogen-only pills, implants, and injections. It also discusses intrauterine devices (IUDs), barrier methods, natural family planning, and sterilization. Effectiveness depends on how the method works and how easy it is to use correctly. Side effects vary by method but can include changes to bleeding patterns, mood changes, weight gain, and risk of ectopic pregnancy if failure occurs. Appropriate medical factors are also outlined for selecting the best contraceptive option.






























































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

















