Downloaded 156 times
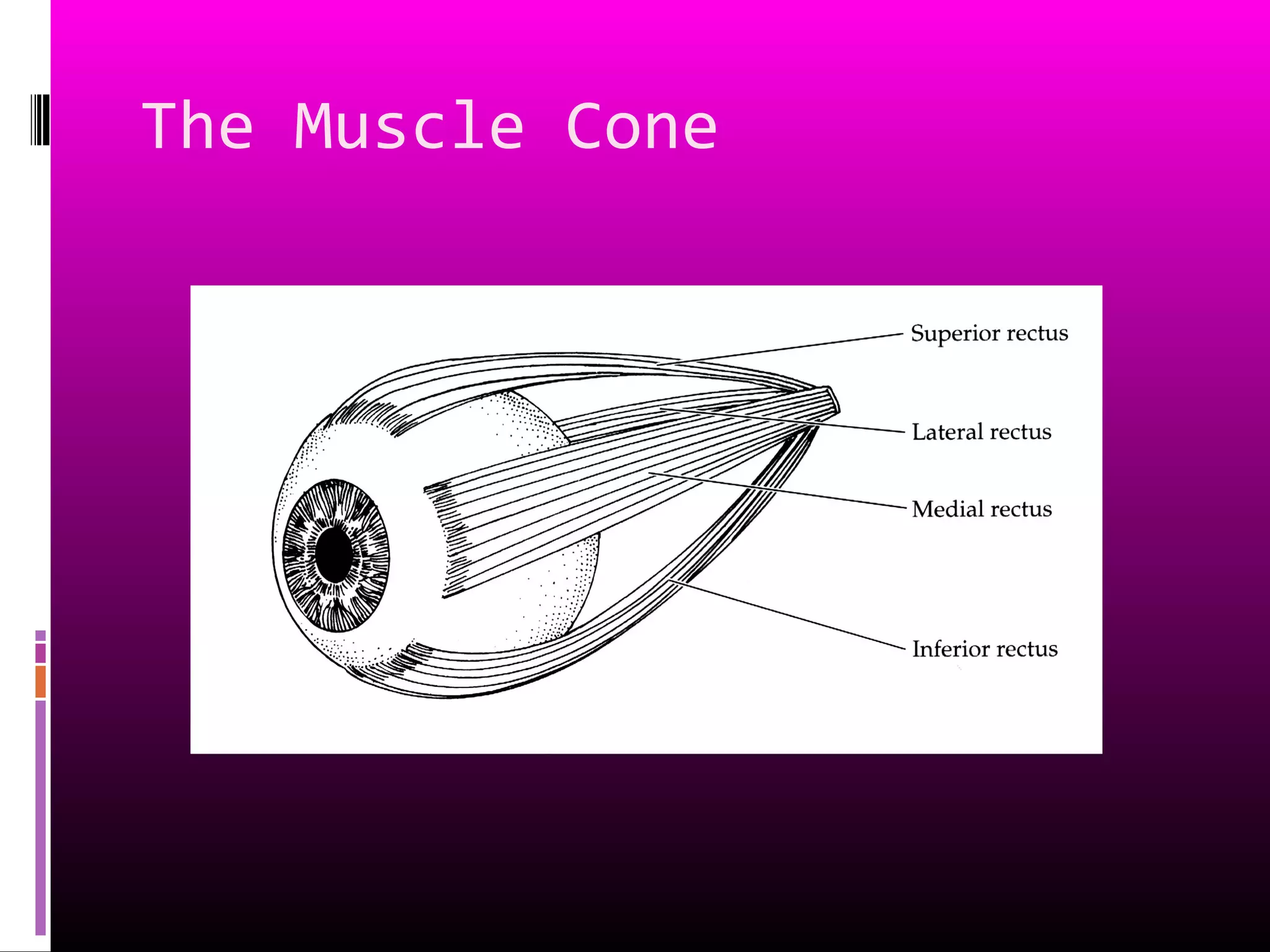

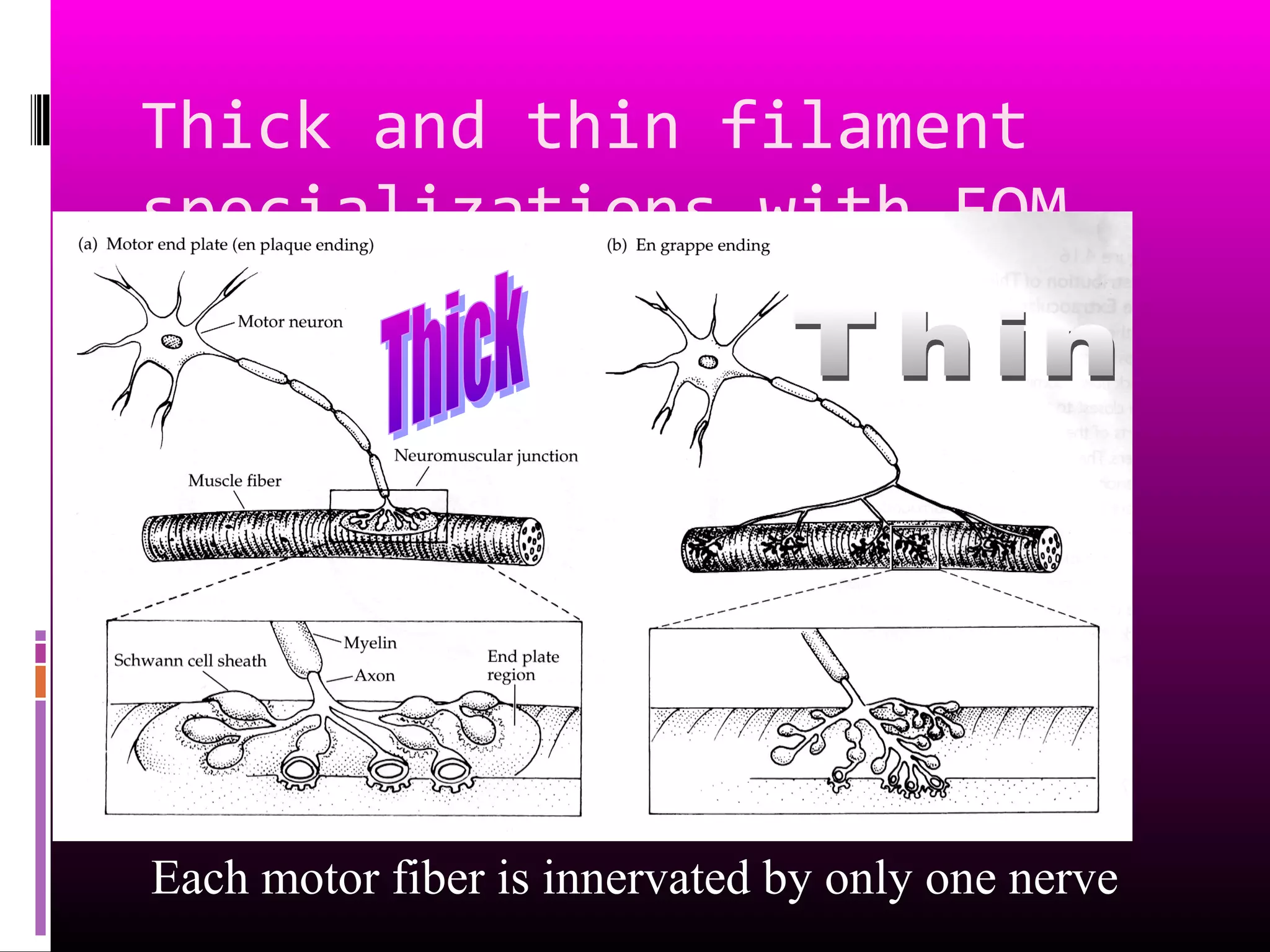
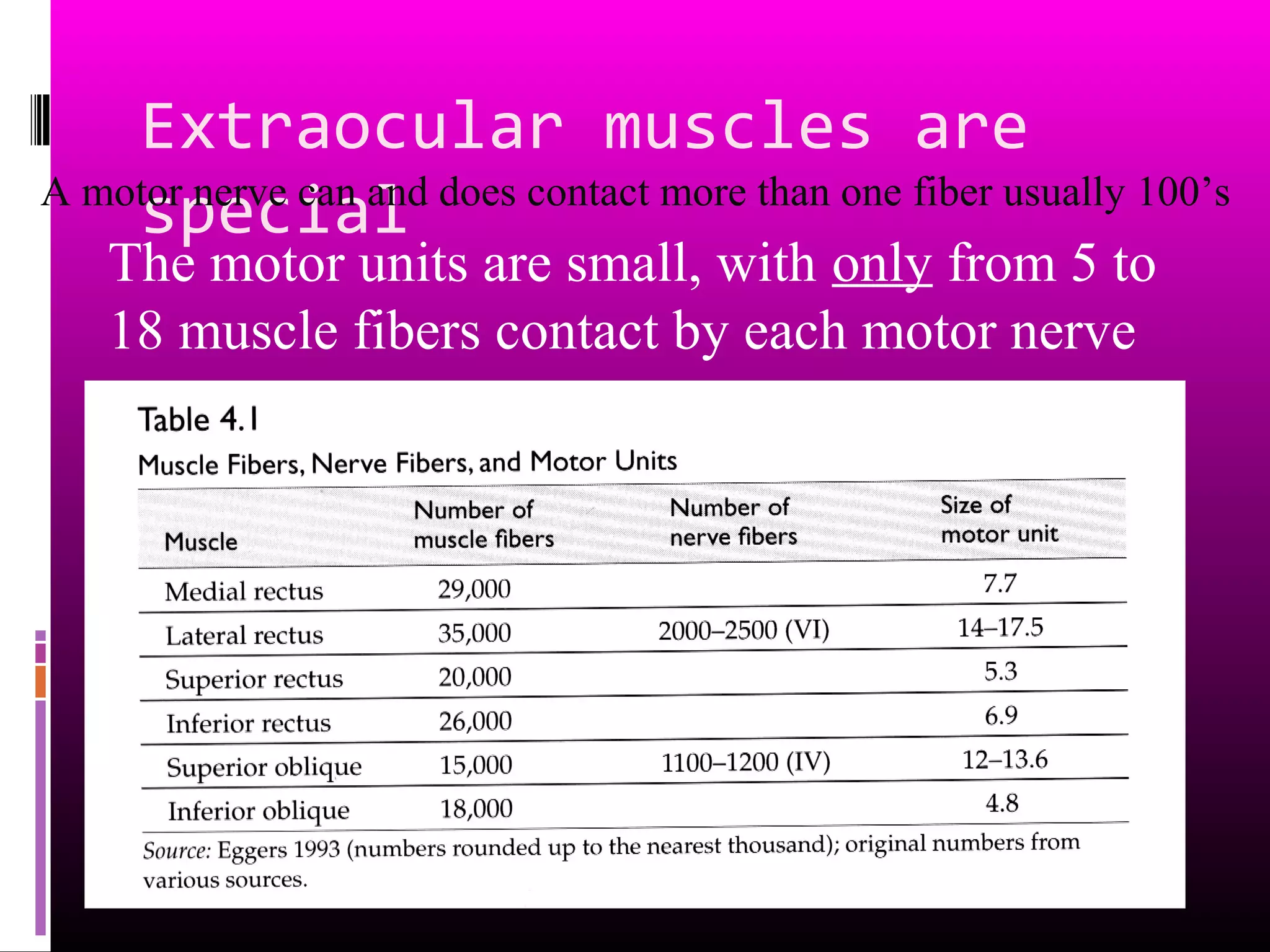

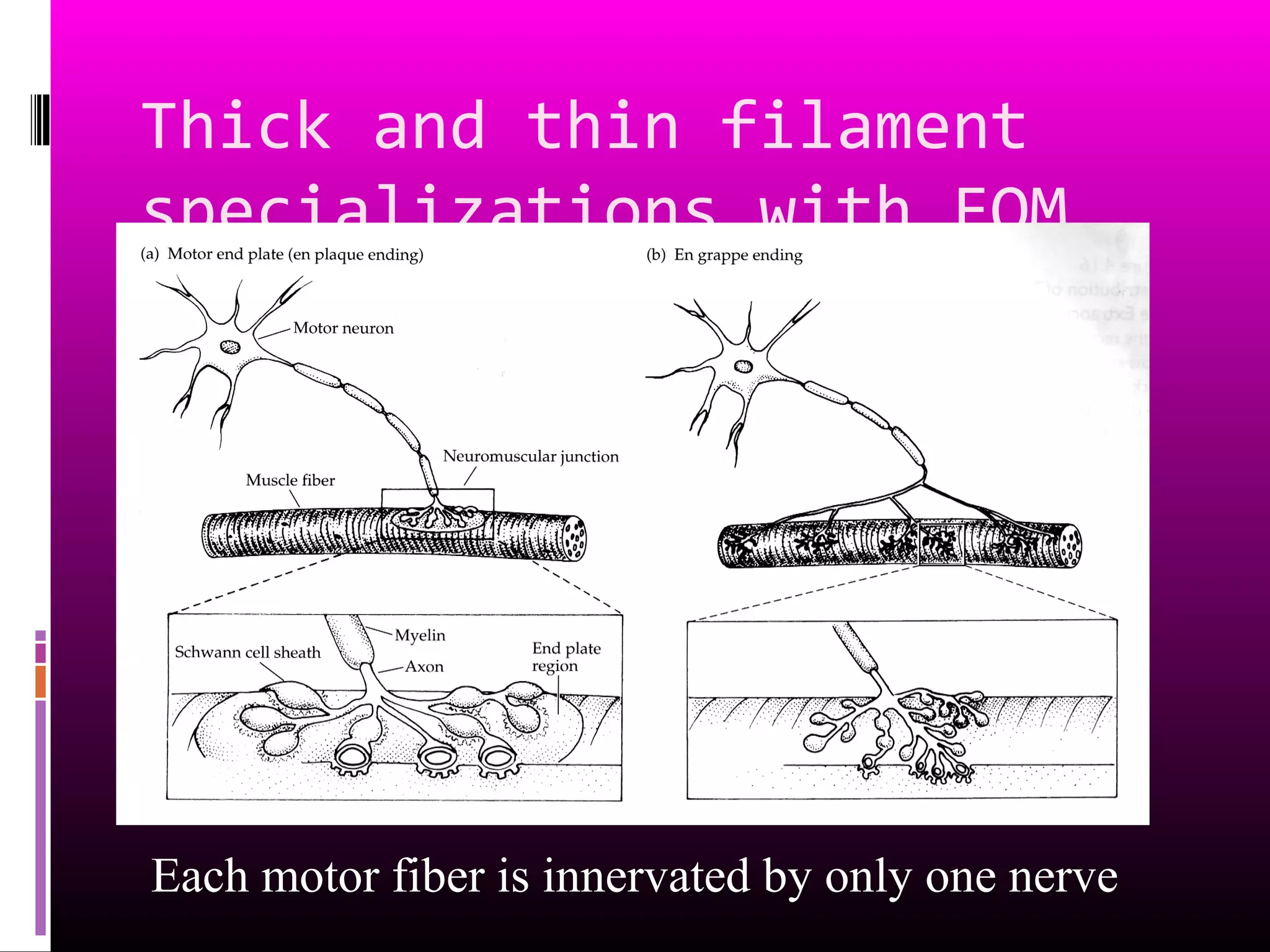
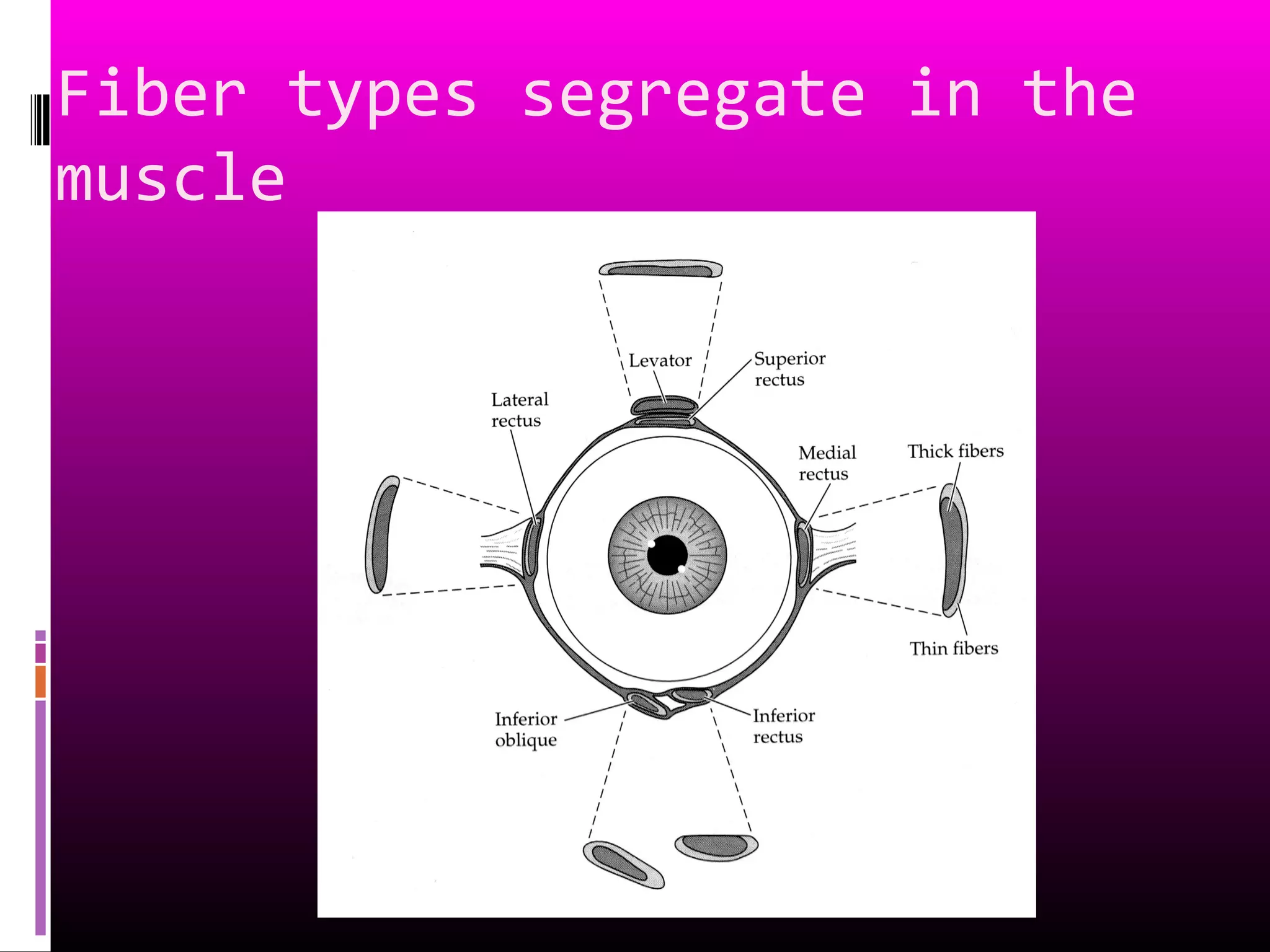
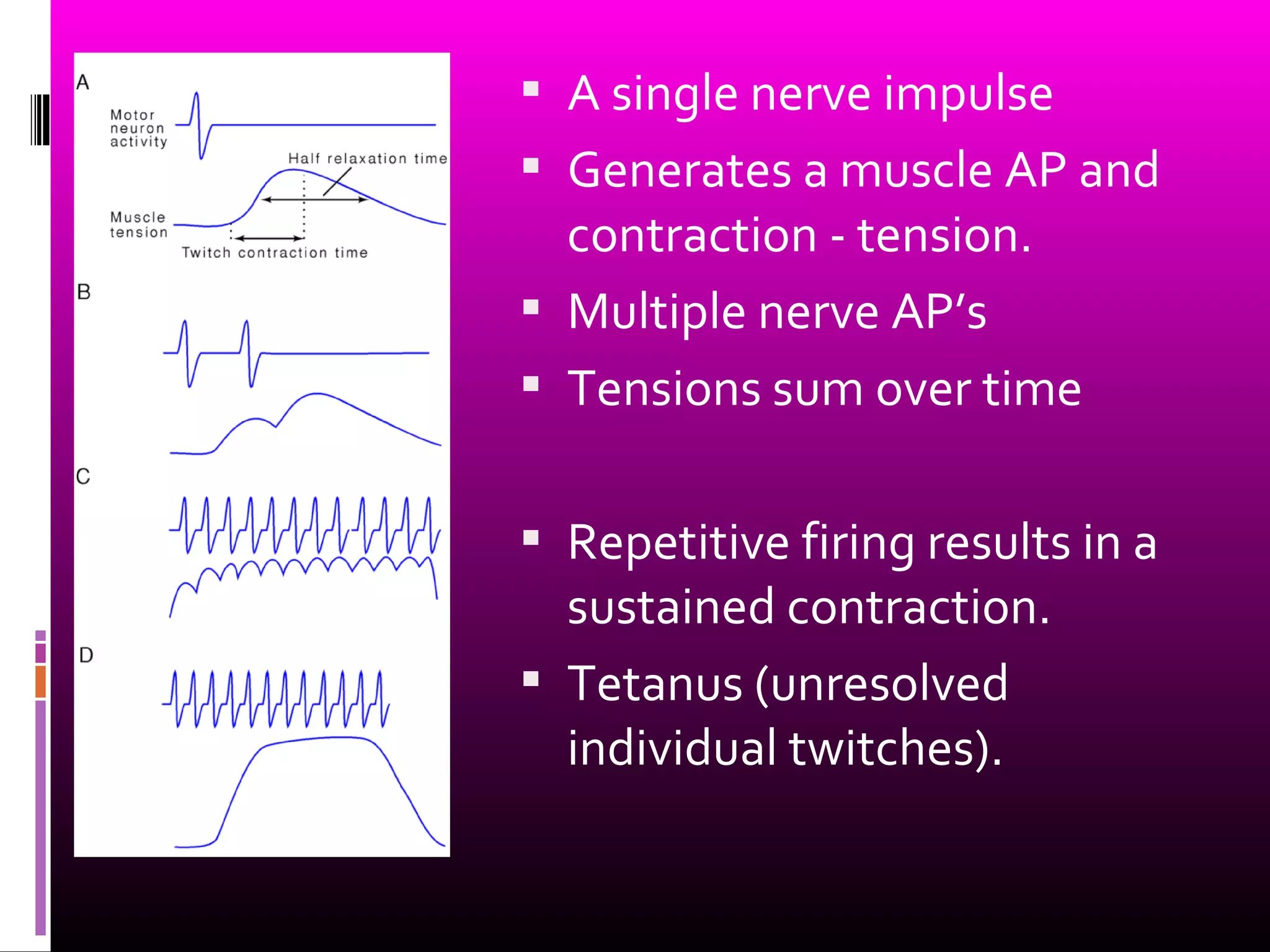
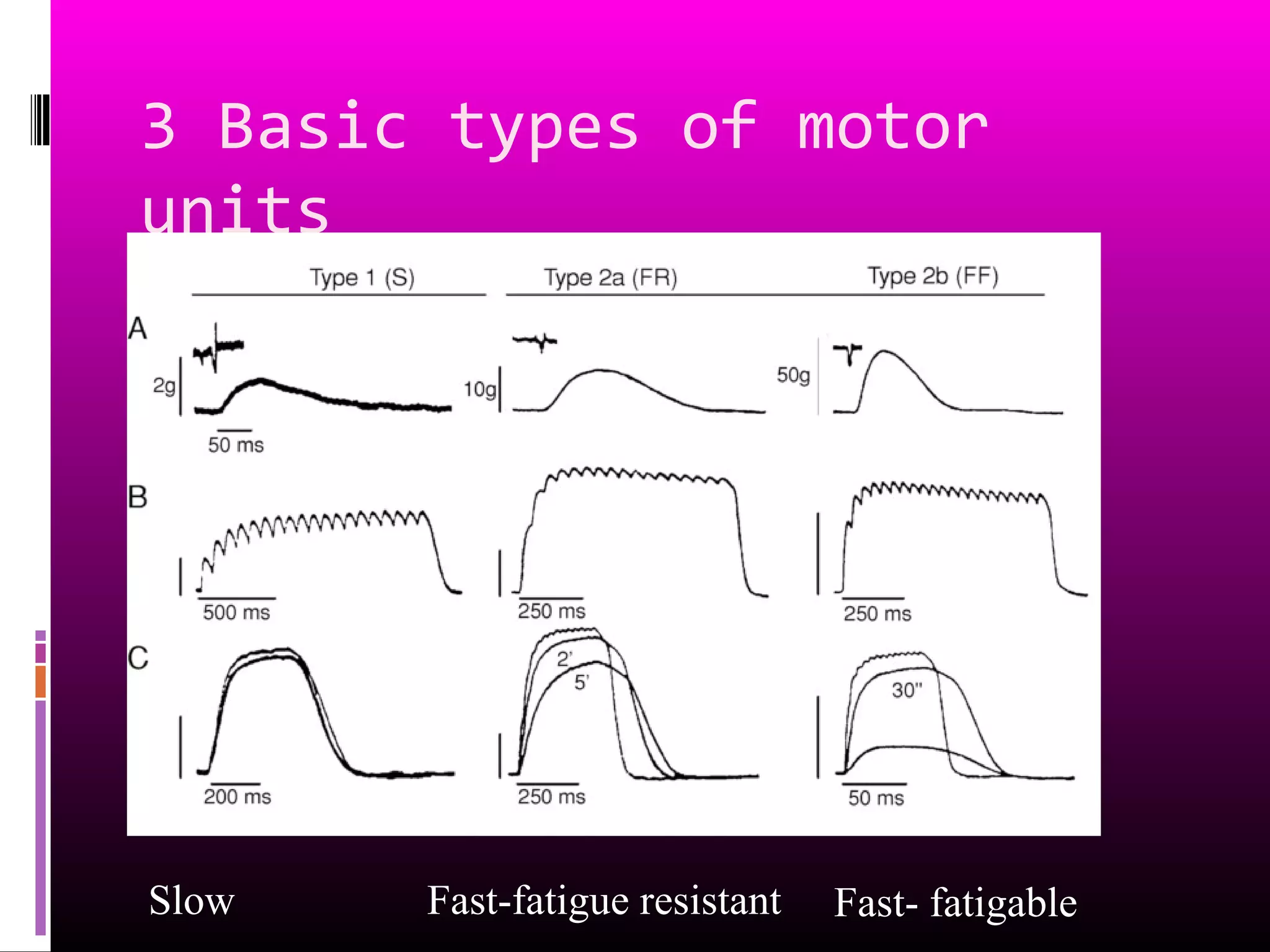
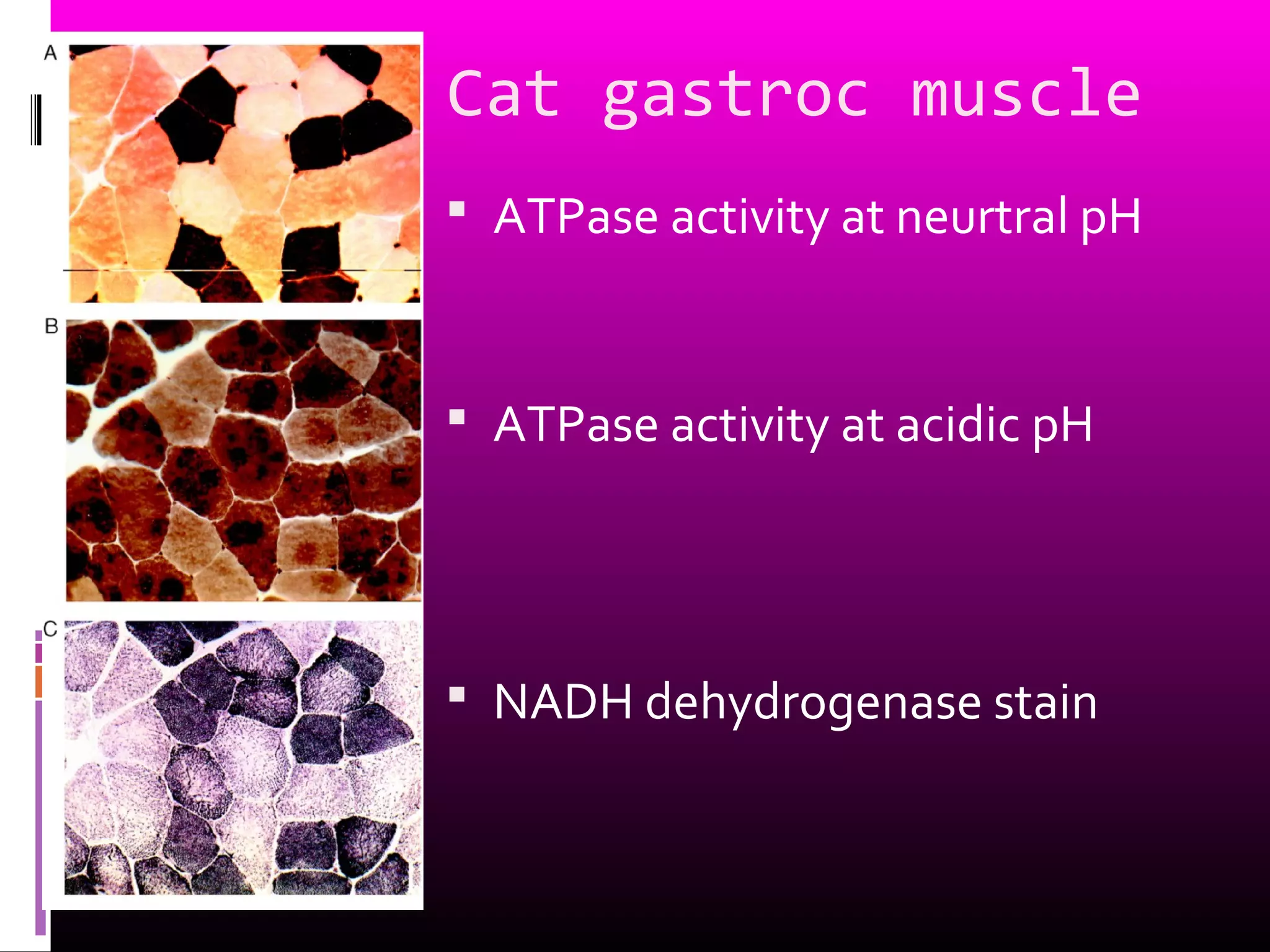

This document discusses eye movements and the anatomy of the extraocular muscles. It describes the different types of eye movements including smooth pursuit, saccades, fixation, and reflex eye movements. It also outlines the actions and innervation of the individual extraocular muscles - the four rectus muscles and two oblique muscles. The document provides details on motor units, fiber types, and recruitment patterns in extraocular muscles.



































































































